The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the
lands and waters on which we live, work and learn.
Aboriginal and Torres Strait Islander peoples should be aware that this website contains images or names of people who have passed away
In this section, we discuss some ideas for self-care. This is an important topic as many conversations that occur in the safety and quality area may be challenging emotionally for everyone involved. The conversations and subject areas may remind people with lived experience of difficult and traumatic personal memories. It is useful to know something about areas that may be challenging for you.
Trauma-informed support and self-care
This approach builds awareness and recognition of the impacts of trauma for consumers, particularly trauma that has been experienced during childhood.
The approach also recognises that many consumers have had traumatic experiences within mental health services. These experiences include service responses that are invalidating, detention, restraint, forced treatment and seclusion.
In addition, many people have experienced trauma in the context of cultural, gender or sexual identity. Colonisation has exposed Aboriginal and Torres Strait Islander people to the impacts of intergenerational trauma: disruptions to parenting and family culture, and experiences of trauma related to forced separation of children from families have had ongoing effects on generations. Many Aboriginal and Torres Strait Islander people have had difficult and challenging experiences when they have accessed health services, including racism, discrimination and adverse events.
Many people with insecure visa status—such as refugees, asylum seekers and culturally diverse people—have experienced trauma and insecurity in their home countries, and during life in refugee camps and immigration processing centres.
One of the key impacts of trauma is that it makes people hesitant and fearful about engaging with mental health services or child health services. A history of trauma can lead people to question themselves—for example, by asking “Is this situation safe or unsafe for me?” Surviving trauma can increase a person’s vigilance and need for certainty and control. Entering or re-entering a mental health service can trigger feelings associated with past experiences, such as fear, danger and strong feelings of vulnerability.
Because lived experience of mental health challenges can be linked with using mental health services, as well as cultural, gender and sexual identity, service providers and engagement leaders must be trauma aware and offer supports for people.
An approach for trauma-informed care
A well-known approach to trauma-informed care was developed by the Substance Abuse and Mental Health Services Administration in the United States. This approach emphasises that services should be aware of the effects and prevalence of trauma, and that services should recognise the signs of trauma in people and populations requiring care. Services should also develop organisational policies, procedures and practices that integrate knowledge about effective trauma care and responses. And services should resist practices that re-traumatise people.26
Challenging topics
When you see an opportunity, or receive an invitation, to be involved in safety and quality, it’s likely that the organisers have considered the best way of involving consumers, carers, families and kinship groups.
Most services employ consumer consultants and Aboriginal and Torres Strait Islander advisers. These people should have guided earlier discussions about the best way to involve people, considering the nature of the proposed topics.
Emotionally sensitive topics can include detailed discussions about adverse events or self-harm when a person was injured or died in care, child safety issues, the experience of restraints and seclusion, and suicide prevention in the service setting. Another area of sensitivity arises when clinicians or specific services are named in complaints processes, which has legal implications. All these factors influence opportunities for involvement and partnership.
Evaluating potential triggers and self-care
Sometimes people with lived experience can experience the language used in safety and quality, and the ways of discussing sensitive topics, as technical, clinical, detached or unwittingly objectifying. However, consumers and carers may not realise all the things that can go wrong in health care, or the various pressures that services are under. They can experience these discussions in unexpected ways, which may be emotionally triggering and distressing.
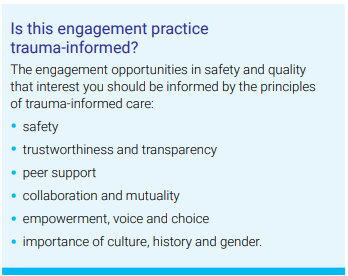
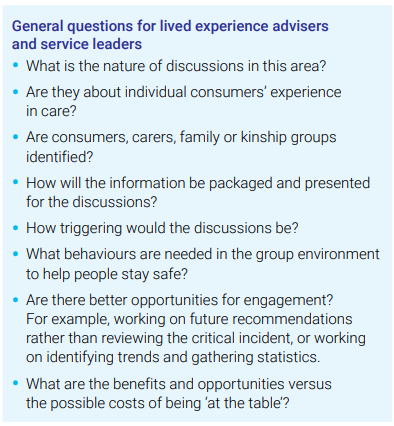
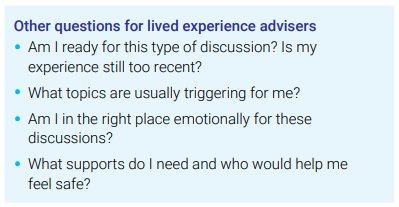
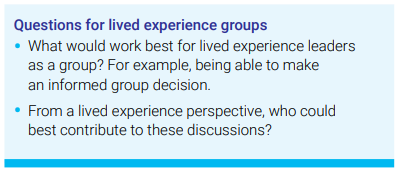
When we were consulting about this guide, lived experience leaders and service leaders suggested that the questions in Table 4 are useful for evaluating triggers and deciding on ways of being involved and partnering.
Table 4: Questions on trauma-informed safety and group engagement
Strategies for self-care from the lived experience perspective
Writing or creating a self-care plan. A plan can help you prepare for your work and remind you when you need self-care. It’s good to prepare your plan before you start working in the group.
Briefing. Ask questions of the contact person or chair as you start getting involved. Find out what’s going to be discussed in the next meeting, and how it will be discussed.
Debriefing. Share your thoughts and responses after meetings with the contact person or chair.
Clarifying any confidentiality matters. Get clear on these matters if you think they will affect your self-care.
Checking in. Talk with other group members, including lived experience members, about how you are handling the subject matter.
Talking to your mentor and support person. Talk about how you are going and your self-care strategies. What practices do they find helpful?
Working out boundaries for your involvement. For example, create limits for your reading and preparation time at home so you have some free times during the day, night or week.
Opt-out strategies. Let group members know that you might need to take a break for self-care during discussions.
Strategies if you are experiencing significant distress
For various reasons, there may be times when you need to prioritise your own mental health over your participation in a safety and quality project; you may need to scale back your involvement for a time. Safety and quality leaders can offer organisational supports to assist you.
Services should have a flexible support system in place to assist representatives and leaders. Ideally, services will:
have a joint understanding with appropriate human resource staff about time for a person’s healing and recovery (if the leader is being paid)
be aware that a consumer may need time away from meeting processes, just like other members of the committee, to address personal or family issues
ensure a variety of ways for all committee members to provide input (e.g. via video, telephone conferencing, email and in writing, as well as in person)
engage in supportive conversations to hear and respond to the person’s views about whether they are able to participate (e.g. the person may decide they are well enough to participate, which should be supported)
ask the consumer to follow up with their doctor if medical clearance is an issue
check in with the person to see if they need assistance to contact supports and services.
Work through the ethics of engaging people with lived experience with consumer consultants and advisers. Have more than one representative involved.
Provide a range of supports to both lived experience members and non-lived experience members of committees and groups, remembering that employees usually have more supports in place, such as employee assistance programs and supervision. Connect lived experience representatives with others (e.g. a meeting buddy).
Encourage all members of the group to have wellbeing strategies as a normal part of caring for themselves, each other and the group as a whole.
Ensure that briefing and debriefing opportunities are available for lived experience representatives. Allow time to check in before and after meetings.
Provide context on quality improvement during discussions, highlighting how specific local issues are related to general trends in safety and quality. Work together to identify the bigger picture of quality and safety improvement.
Consider safety issues around culture, gender and age. How do these issues affect discussions and lived experience representatives?
Clarify confidentiality boundaries to ensure that representatives can speak with mentors and support people.
Plan meetings well: find ways to present difficult information that help protect and create boundaries for group members. Clarify the purpose and ways of working together.
Use safe and respectful language. Model respectful language and behaviour for group members. This acknowledges the distress that people involved in discussions of particular topics may have experienced.
Follow practices for a welcoming, inclusive culture, as detailed in Section 4.
Last updated:
Acknowledgement of Country
The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the lands and waters on which we live, work and learn.
Diversity
The Commission is committed to embracing diversity and eliminating all forms of discrimination in the provision of health services. The Commission welcomes all people irrespective of ethnicity, lifestyle choice, faith, sexual orientation and gender identity.
Lived Experience
We acknowledge the individual and collective contributions of those with a lived and living experience of mental ill-health and suicide, and those who love, have loved and care for them. Each person’s journey is unique and a valued contribution to Australia’s commitment to mental health suicide prevention systems reform.