The Commission acknowledges and pays respect to the past and present Traditional Custodians and Elders of this nation and the continuation of cultural, spiritual and educational practices of Aboriginal and Torres Strait Islander peoples.
Aboriginal and Torres Strait Islander peoples should be aware that this website contains images or names of people who have passed away
The National Children’s Mental Health and Wellbeing Strategy Report
1.1 Why this Strategy is so important
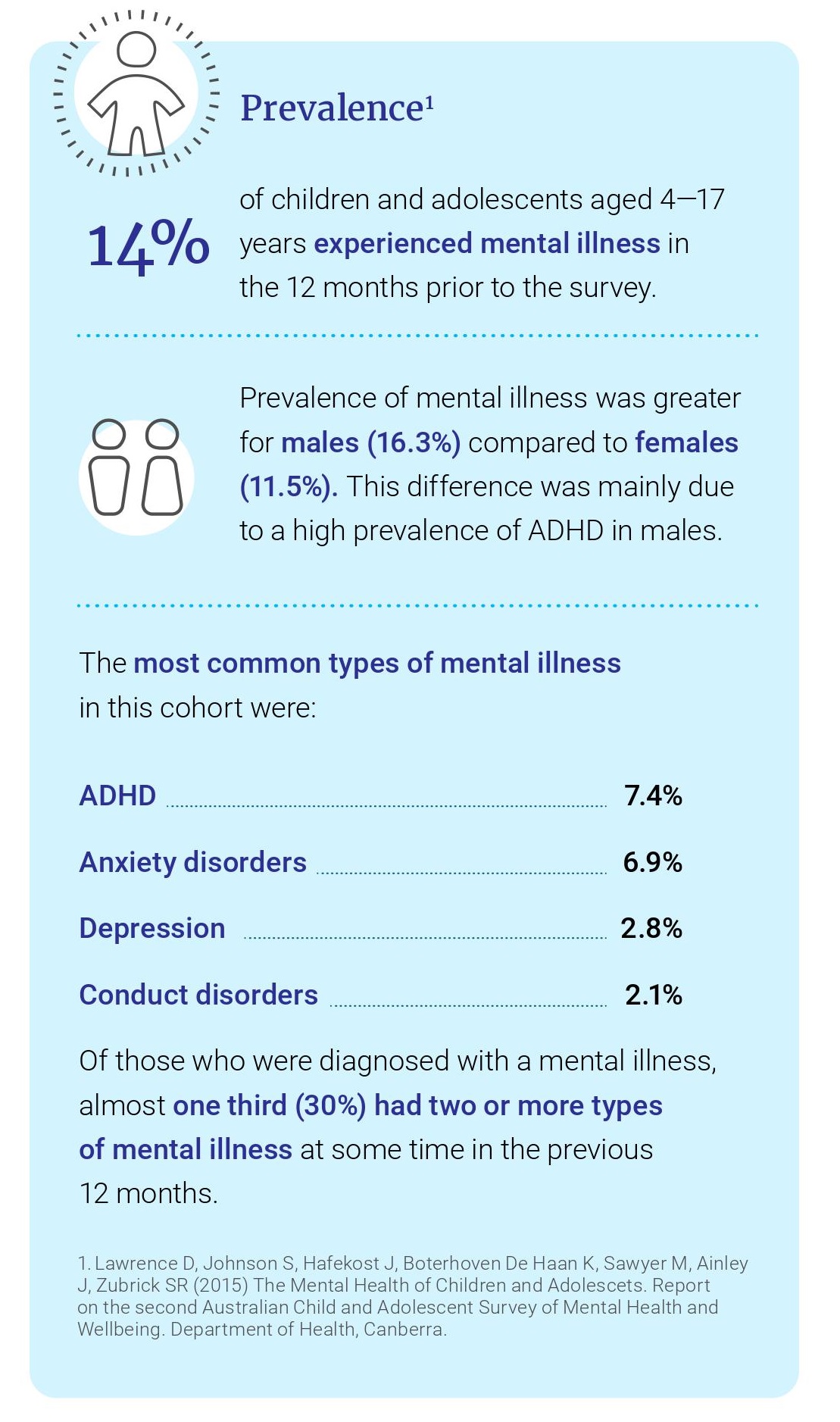
This National Strategy is critical because mental health struggles often begin during childhood. An estimated 50% of adult mental illness begins before 14 years of age. In 2015, anxiety, depressive disorders and conduct disorders accounted for three of the five leading causes of disease burden for children aged 5-14 years. Furthermore, there is evidence that poor mental health during childhood can lead to long term struggles. One study found that 50% of children with mental illness continue to struggle in adulthood; while the other 50% no longer warranted a diagnosis, their chance of functioning well was still less than that of people without a history of mental illness during childhood.
It is relatively common for children to experience or be at risk of experiencing poor mental health. Evidence indicates the first 2000 days of life are a critical period, and interventions during this time can result in significant improvement to children’s early life experiences, health and development. This Strategy recognises the importance of supporting children from infancy, particularly through empowering parents, carers and communities. Estimates indicate that 8% of infants (0–1 years) have 5 or more risk factors for developing mental illness, increasing to 20% of 10—11-year-olds.
While genetic factors contribute to mental illness, there are strong links between adverse childhood experiences (ACEs) and development of mental illness. Such experiences typically include violence, sexual abuse, neglect, and other kinds of household dysfunction, including alcohol and substance abuse. Challenging circumstances such as parental separation and divorce may also be included. It is estimated that about 2.5 million Australian adults (13%) experienced physical and/or sexual abuse during childhood. The issue of domestic and family abuse warrants a dedicated standalone national response and matching actions, beyond the scope of this strategy alone.
Another prominent ACE is Foetal Alcohol Spectrum Disorder (FASD). FASD is a diagnostic term for a range of physical, cognitive, behavioural and neurodevelopmental impairments resulting from maternal drinking during pregnancy. While prevalence of FASD in Australia is difficult to determine, the global prevalence of FASD among children and youth in the general population was estimated to be 7.7 per 1000 population. Children with FASD are significantly more likely to have a mental illness and have an average life expectancy of 34 years of age. There are also lifelong effects including secondary impairments such as difficulties accessing education and maintaining employment, increased substance use, and increased contact with the justice system. The Australian Government developed the National FASD Strategic Action Plan 2018-2028, which aims to reduce the prevalence of FASD and identifies priorities for action. The national priorities include prevention, screening and diagnosis, support and management, and priority groups and populations at increased risks.
Exposure to ACEs is common, and they tend to cluster within families, but there are clear actions that can be taken to mitigate them, both by mental health professionals and through action in other domains outside of health care. These actions include instigating wrap around services at parent, family and community level.
The economic value of supporting mental health during childhood has also been demonstrated – it costs significantly more to treat mental illness in adolescence and adulthood than it does to promote mental health and, if needed, intervene early during childhood. One report found the cost to government of late intervention in Australia is $15.2bn each year. Economic evaluations of early childhood development programs have repeatedly shown that the benefits exceed the costs. This has been demonstrated in the United Kingdom, with school-based social and emotional learning programs to prevent conduct disorders in the UK demonstrating cost savings of £150,000 for severe problems and £75,000 for mild problems (for each case prevented). Similarly, one Australian report found that the return on investment of parenting programs for the prevention of childhood anxiety disorders was $2.40 for every $1 invested.
Not only is this Strategy critically important, but it’s critically needed now. Many experts have described Australia’s current child mental health system as “broken”. While there is currently no regular national system for monitoring and reporting on the overall mental health and wellbeing of children 0-12 years old, there are a small number of data sources to assist our understanding of the current landscape. Data from the Australian Child and Adolescent Survey of Mental Health and Wellbeing indicates that one in seven Australian children aged 4-17 years’ experience mental illness (see above).
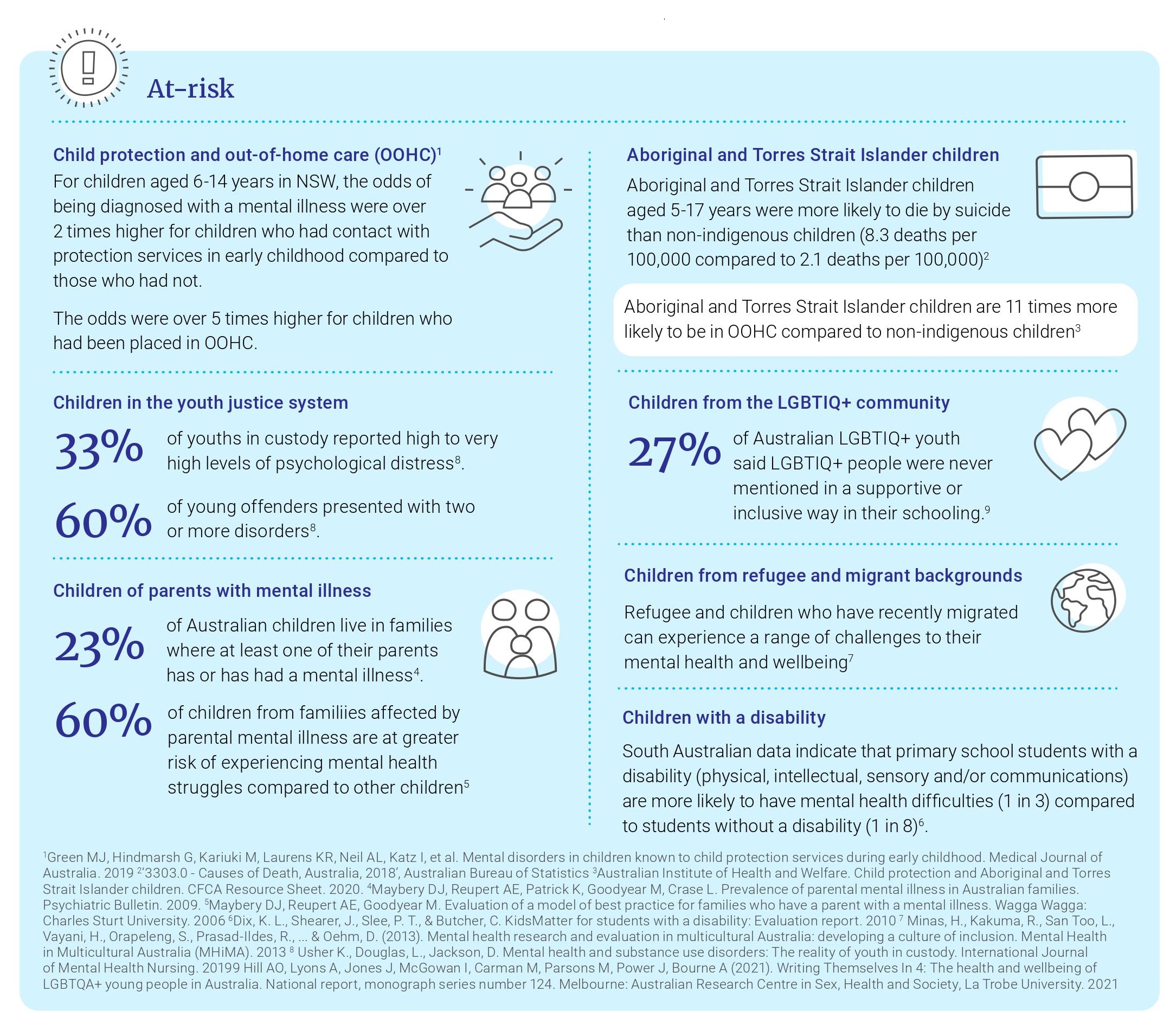
The above figures refer to Australian children generally. Some cohorts of children are known to be at increased risk of experiencing mental ill health, including:
Children who have experienced the child protection and out-of-home care system. This may be as a result of exposure to trauma prior to involvement with child protection services, as well as ongoing stress while in the care system.
Aboriginal and Torres Strait Islander children. The wellbeing of Aboriginal and Torres Strait Islander populations continues to be significantly impacted by collective trauma, including from experiences of the Stolen Generations, disempowerment, and cycles of disadvantage.
Children of parents with mental ill health or parents with substance use problems. Parental mental illness can place families at a greater risk of experiencing physical, emotional, and financial problems. Families with parental substance misuse have higher rates of neglect, which is a major factor in a child being brought into care.
Research also indicates that children of parents with substance use problems are significantly more likely to develop alcohol and drug use disorders than their peers.
Children with disability or chronic illness. Children with a disability or a chronic illness are at significantly higher risk of having mental health issues.
Refugees and children who have recently migrated. The migration experience can negatively impact child mental health and wellbeing, given the higher likelihood of exposure to trauma and stress of adapting to new culture and language, and in some cases with uncertain legal status and fear of deportation.
Children who identify as LGBTQI+ or have a family member, parent or carer who does. For gender diverse children who are not supported by gender affirming care there is an increased risk of depression, anxiety and suicidality. Wellbeing may also be impacted when children experience stigma relating to a family member identifying as LGBTIQ+.
Children who are, or have been, incarcerated as part of the youth justice system.
Among these cohorts of children who are more likely to struggle, if support is absent or provided too late, the individual, social and economic consequences are severe. Children in care are less likely to continue their education beyond the minimum age requirement, and are more likely to attend numerous different schools with lower attendance rates overall. There is also research that young people who have been involved in the child protection system (due to abuse or neglect) are subsequently more likely to be homeless and to engage in criminal activity than those who were not. Children who have had contact with the youth justice system experience more mental health disorders and substance use disorders than the general population. Despite the high prevalence of poor mental health for young people in custody, they are excluded from MBS subsidised primary care for the development of a mental healthcare plan and MBS subsidised mental health care.
For children of parents with mental ill health, caring responsibilities can conflict with age-appropriate activities and school attendance. There is also evidence of lower levels of attainment in terms of communication, academic competencies and social function in children whose parents have high levels of psychological distress.
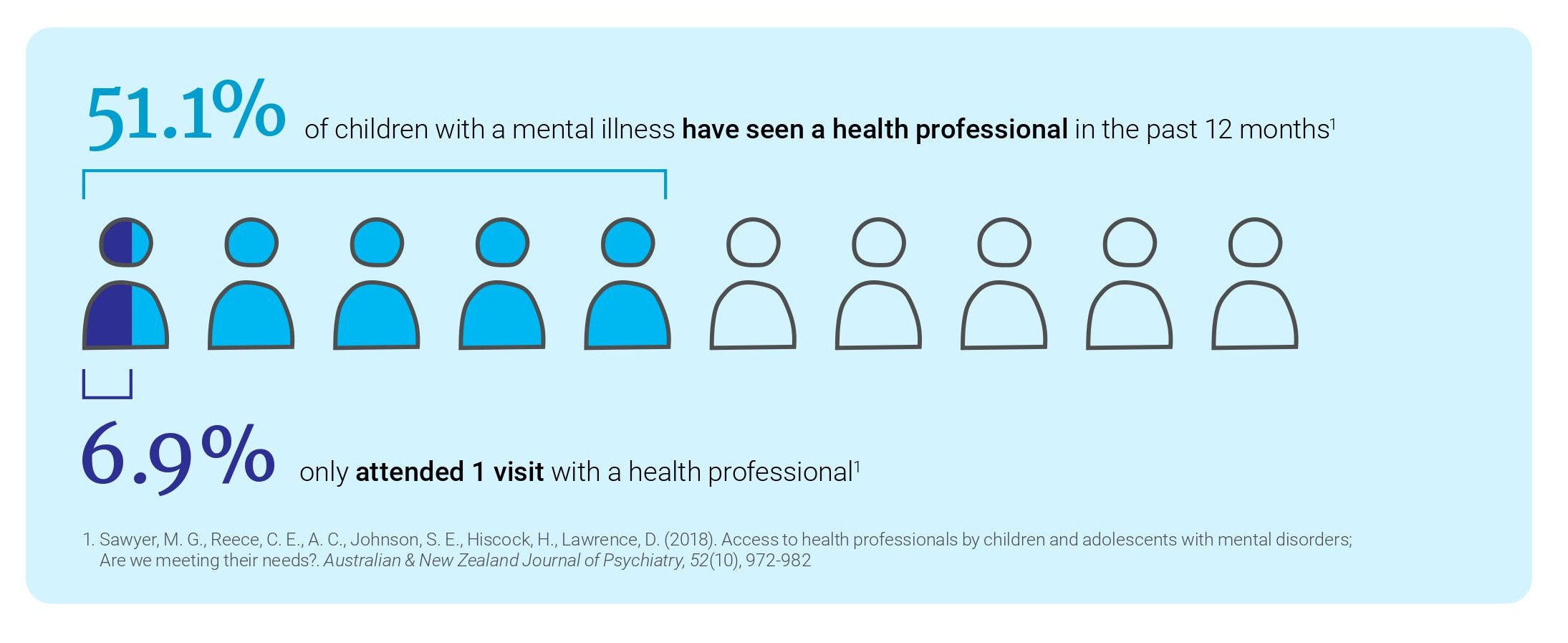
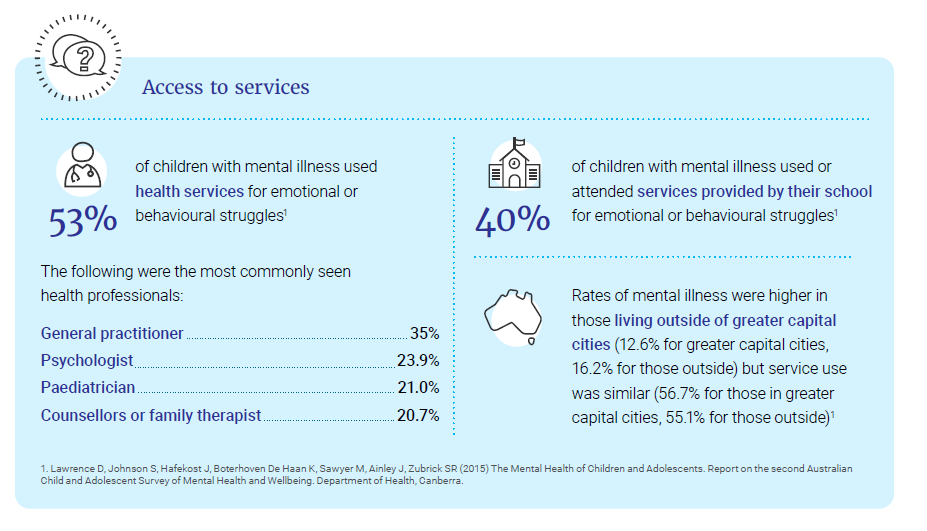
The supports that are available are not consistently reaching the children and families who are struggling. Data from the Australian Child and Adolescent Survey of Mental Health and Wellbeing Study indicates that only around half of all children who experienced mental illness in the last 12 months had accessed services, and less than a third of parents used services to help support their child who was struggling. There is evidence that the majority of children with mental illness in Australia do not have enough contact with health professionals to allow for minimum standards of treatment to be provided. A study involving 846 children aged 4-17 years found that almost half (48.9%) of those with mental illness had not accessed any services in the past 12 months.
In addition to ‘dosage’ shortfalls, the quality of service contacts is also not consistently high – adherence to assessment and management guidelines is also low, with one study finding that rates were 33% for depression and 54% for anxiety, in the context of care for children 15 years and under. So even where children are able to access services, it cannot be guaranteed that they are receiving evidence-based treatments.
Children’s mental health appears to be underserved when compared to older age groups. The Australian Child and Adolescent Survey of Mental Health and Wellbeing found that the prevalence of mental illness was similar between those aged 4-11 years and those aged 12-17 years at 13.6% and 14.4%, respectively. However, the survey found that of children with mental illness, those aged 4-11 years were less likely to access a health service provider for emotional or behavioural concerns (46.3%) than young people aged 12-17 years (60.7%).
For contact with specialist mental health services, data indicate that many more services are delivered to 12-24 years (> 4 million) than to children under 12 (552,000), with less than 1% of 0-4 year olds and less than 6% of 5-11 year olds receiving a service in 2014-15. Rates of spending on the MBS Better Access program are similarly low, at only 5.6% of the total scheme for children under 12 years of age in 2015-16. Although it appears that service access may also be low for children aged 0-4 years, there is limited data available about the prevalence of social and emotional difficulties experienced in this age group.
Reasons for insufficient access to services could include:
lengthy waitlists mean children can’t access services when they need them
the services or supports children need simply don’t exist or are not known to the family
the child is refused support from a service because they don’t meet severity thresholds or don’t have a confirmed diagnosis
poor mental health literacy and a lack of awareness of risks amongst parents and teachers
stigma around mental health, parenting programs and service access
out-of-pocket costs for a service
a lack of specialist workforce to meet the needs of children and families.
For rural and remote communities, there are even greater barriers to access. Around 30% of all Australian children aged 0-14 live in rural areas, and 3% live in remote and very remote areas. For many, the nearest services are located in major hospitals a long distance away, and to see a service provider face to face, a round trip of 200km would not be unusual.
The number and type of practitioners able to work therapeutically with children and families is not clearly defined, and in rural and remote areas, is unlikely to include the full range of clinical and allied health practitioners such as speech pathology and occupational therapy, given known issues of workforce maldistribution. While some workforce data concerning psychologists and psychiatrists with child mental health and wellbeing related endorsement are available, ascertaining the full breadth of the workforce and its distribution (mapped according to need) is difficult.
Amongst professionals who work with children more broadly, including those in the health, social, disability and community sectors, there is variability in the level of mental health training, supervision, and continuing professional development that they have received. In response, the National Workforce Centre for Child Mental Health was recently established, with the aim of assisting professionals, service systems and organisations that work with children to develop their capacity to identify, assess and support children at risk of mental health difficulties.
Last updated:
Acknowledgement of Country
The Commission acknowledges Aboriginal and Torres strait Islander peoples as the Traditional Custodians of the lands and waters on which we live, work and learn.
Diversity
The Commission is committed to embracing diversity and eliminating all forms of discrimination in the provision of health services. The Commission welcomes all people irrespective of ethnicity, lifestyle choice, faith, sexual orientation and gender identity.
Lived Experience
We acknowledge the individual and collective contributions of those with a lived and living experience of mental ill-health and suicide, and those who love, have loved and care for them. Each person’s journey is unique and a valued contribution to Australia’s commitment to mental health suicide prevention systems reform.