The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the
lands and waters on which we live, work and learn.
Aboriginal and Torres Strait Islander peoples should be aware that this website contains images or names of people who have passed away
The National Children’s Mental Health and Wellbeing Strategy Report
2.2 Wellbeing continuum
To support the cultural shift this Strategy aims to achieve, we have adopted a continuum-based model of mental health and wellbeing, with non-stigmatised language characterising the various experiences of wellbeing (see Box 1 below).
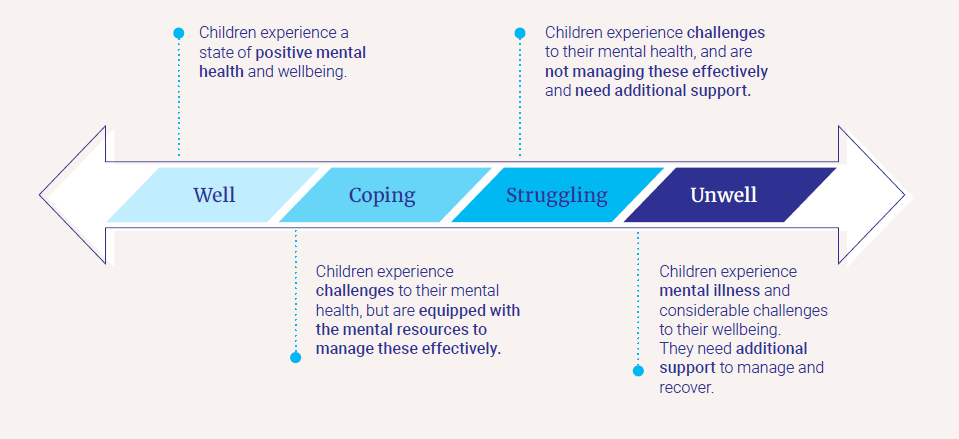
Box 1: A mental health and wellbeing continuum
Children’s emotional experiences cannot always be distinctly defined as well or unwell, as there are varying levels of mental health and wellbeing. Therefore, it is more accurate to describe emotional experiences as falling along a continuum. The figure below outlines the continuum model of mental health used to guide this Strategy.
The continuum approach highlights that there are opportunities to promote improved wellbeing and possibly intervene before a child becomes unwell. It also acknowledges that a child may have a diagnosed mental illness, but function well socially and educationally (i.e. ‘coping’). Similarly, a child who is ‘struggling’ would not require a diagnosis, but would be experiencing a decline in their usual functioning or anticipated developmental trajectory.
The optimal mental health system includes universal services and programs that help children remain in, or move to, the well end of the continuum. In addition, it would provide targeted supports and services for children who are struggling. This Strategy proposes that children should be able to access funded services at the point that they are beginning to struggle, rather than only once they are unwell and have received a diagnosis.
This description of mental health and wellbeing also introduces terminology that is more approachable than the traditional language of ‘mental health’ and ‘mental illness’, which can be stigmatised and not well understood. As such, structuring a system around this continuum offers a common language to help families, health professionals and educators to discuss children’s emotional wellbeing.
Consultations also found that this continuum approach aligns well with Aboriginal and Torres Strait Islander concepts of social and emotional wellbeing , which focus less on mental illness and more on holistic approaches to supporting wellbeing.
Future work will be necessary to embed a wellbeing continuum approach
While the introduction of the continuum concept appears to have widespread support, the question of the most appropriate words to use at the four anchor points is still the subject of debate, as is the question of whether to introduce a fifth anchor point - 'thriving’. It is suggested that thriving reflects not only the absence of psychological or behavioural problems, but also the presence of strengths and wellness.
Thriving can be viewed as a core set of life skills essential to emotional regulation, social participation and global citizenship. The EPOCH model (outlined below) suggests that thriving has 5 dimensions:
Engagement — the capacity to become absorbed in and focused on what one is doing, as well as involvement and interest in life activities and tasks. Very high levels of engagement have been referred to as “flow”.
Perseverance — the ability to pursue one’s goals to completion, even in the face of obstacles.
Optimism — is characterised by hopefulness and confidence about the future, a tendency to take a favourable view of things, and an explanatory style marked by evaluating negative events as temporary, external, and specific to the situation.
Connectedness — the sense that one has satisfying relationships with others, believing that one is cared for, loved, esteemed, and providing friendship or support to others. For Aboriginal and Torres Strait Islander children and families, thriving may also mean connectedness to Aboriginal culture and identity.
Happiness — is conceptualised as a relatively steady state of positive mood and feeling content with one’s life, rather than a momentary emotion.
We recognise that language is important in this context, and that the words used for the anchor points along the continuum need to be carefully considered. Further work to address this is warranted, and we would encourage this to be done in an empirical manner by systematically eliciting the views of stakeholders, children and families, and professionals. Additionally, further work should be undertaken to understand how a continuum approach could best be operationalised in the service system, particularly with regards to clinical requirements for diagnostics.
Notwithstanding the challenges above, we want to advocate for language that recognises that mental health is experienced on a continuum, and that a diagnosis should not be a prerequisite to supporting children who are struggling with their mental health and wellbeing.
Last updated:
Acknowledgement of Country
The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the lands and waters on which we live, work and learn.
Diversity
The Commission is committed to embracing diversity and eliminating all forms of discrimination in the provision of health services. The Commission welcomes all people irrespective of ethnicity, lifestyle choice, faith, sexual orientation and gender identity.
Lived Experience
We acknowledge the individual and collective contributions of those with a lived and living experience of mental ill-health and suicide, and those who love, have loved and care for them. Each person’s journey is unique and a valued contribution to Australia’s commitment to mental health suicide prevention systems reform.