The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the
lands and waters on which we live, work and learn.
Aboriginal and Torres Strait Islander peoples should be aware that this website contains images or names of people who have passed away
The National Children’s Mental Health and Wellbeing Strategy Report
Focus area 2: The Service System
The current service system (both health and social services) is in great need of reform. Access to mental health services does not currently match the needs of children aged 0-12 years. There are:
unclear and inadequate entry points for services
unhelpful requirements for a clinical diagnosis before treatment is provided
lack of services available after hours or at affordable rates
structural barriers that feed a disconnect between primary services (such as GPs) and mental health services.
If families recognise the need for professional help, the system is hard to navigate for both families and professionals. The service system is not oriented to intervene as early as possible and does not target factors that increase a child’s vulnerability. There can be long waits or high thresholds of severity, resulting in services focusing on acute and critical responses well after the emergence of a child’s struggles. Some services only focus on particular diagnoses despite the knowledge that comorbidity is very common and intervening before a child warrants a diagnosis may be more effective.
While mental ill health is common across Australia, Australians living in rural and remote areas access services at a much lower rate. In 2016-17 people living in remote areas accessed MBS funded mental health services at a rate of 81 service encounters per 1000 people, compared with 495 encounters per 1000 people in major cities. This may be due to a number of factors, including limited access to services and inequitable workforce distribution.
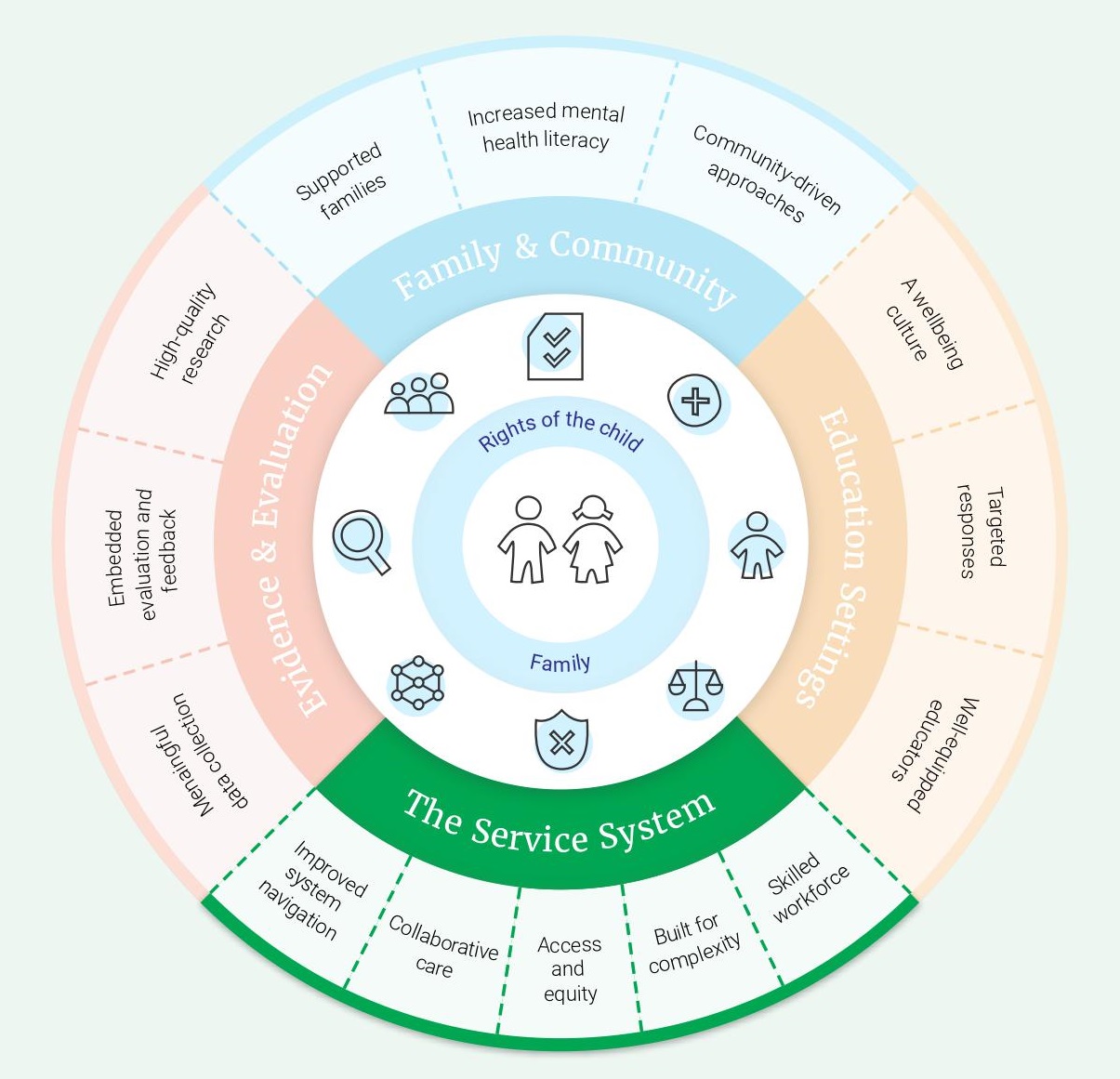
The Service System objectives:
2.1. Improved system navigation
2.2. Collaborative care
2.3. Access and equity
2.4. Built for complexity
2.5. Skilled workforce
Objective 2.1 Improved system navigation
Responsibility for finding the right supports often falls to parents to act as system navigators for their child. Families often feel daunted and lost as they try to find and access the services they or their child need. There is often a sense of ‘luck’ when families connect with the right services for them, or they happen to have been in the ‘right conversation at the right time’. This means that many families are likely to be unfairly missing out to their detriment. The element of luck needs to be removed from the system so that families consistently get the services they need when they need them.
One study suggested that less than half (44%) of parents are confident in knowing where to go for professional help if their child is experiencing mental illness. There is a lack of clear information about where they can access support for their children. As a result, families seek information about available supports through various channels, including via other parents, schools, or health professionals (for example, GPs or paediatricians). A lack of clear, consistent information about where to seek help delays access to services and creates additional stress and burden for families (action 2.1.a).
The current system is fragmented. There is lack of coordination between various sectors, jurisdictions and organisations involved in supporting children’s mental health and wellbeing. Even when professionals (such as early childhood educators, maternal child and family health nurses, or GPs) identify that a child is struggling, there are not clear pathways for referring families to appropriate care. As an example of the complexity of the service landscape, recent service mapping in Victoria identified Commonwealth and State Government programs and service types. It is incredibly difficult for service providers to navigate this many options, let alone for a family in distress. There are also poor connections when families move across regions or interstate and want to connect with equivalent services in the new location (action 2.1.b). PHNs have a role in improving this system navigation for children and families.
In addition to the difficulties navigating the sheer number of options, the services are not organised in a way that provides a logical pathway for care. For example, there can be a disconnect between assessment services and treatment services, such that many publicly funded multidisciplinary programs provide assessments only. The typical trajectory for a child who is struggling often involves a series of sequential assessments punctuated by long waiting times before a care plan and/or diagnosis can be formulated (action 2.1.c). The proposed model of integrated child and family wellbeing services (page 47-49) describes a model for addressing this and other systemic issues for children and families seeking support and care. It may be appropriate, in some cases, for services to require an accurate diagnosis prior to beginning treatment. However, there should always be supports put in place to begin meeting the child’s need, even when waiting for a diagnosis to be confirmed.
Similarly, age thresholds for different services don’t allow smooth transitions in care from childhood into adolescence, and later into adulthood. For example, infant mental health (0-4 years) can be a source of relatively consistent care via a single service, however children are then ineligible to continue with the service when they reach school age. For young people who have been receiving care via Child and Adolescent Mental Health Services (CAMHS), the shift to adult mental health services can be jarring. The timing of transition is often seen by young people as arbitrary and misaligned with their needs and developmental stage (action 2.1.b). More consideration must be given as to how policy, services and implementation will ensure a seamless transition from childhood to adulthood in the healthcare system (action 2.1.d).
The lack of clarity around where and how to access supports also makes it more challenging to identify service gaps. Families may be looking for services that aren’t available in their region, or that they are ineligible for due to strict entry criteria. As system fragmentation is addressed, work should be undertaken to model the current and future demand for mental health services and identify gaps (action 2.1.e).
Things we can build on
HealthPathways is an online health information portal for GPs to be used at the point of care. It is an example of an approach that has been used to assist clinicians to make assessments and referrals in a range of areas of health including suicide prevention and routine antenatal care. Rather than traditional clinical guidelines, ‘pathways’ in the online portal are developed through locally-based expert consensus to reflect agreements between primary and specialist services about how individuals with particular conditions will be managed in the local context. As well as supporting a consistent and best-practice referral approach, HealthPathways also offers cost savings through reductions in unnecessary referrals. At this point, not all regions are using HealthPathways and/or may not have pathways established for children’s mental health. Also, HealthPathways is typically only accessible by GPs (and some hospitals), but not other service providers or families in the community.
Aboriginal and Community Controlled Health Organisations (ACCHOs) are primary health care services initiated and operated by local Aboriginal communities. Their model involves holistic interdisciplinary care and is distinct from traditional health services as it responds to health at the individual, family and community health level.
A typical ACCHO may offer an array of clinical services delivered by GPs, practice nurses, midwives, child health nurses, dentists, drug and alcohol workers, psychologists, psychiatrists, pharmacists, dietitians and podiatrists. This is often coupled with a social support team to provide social and emotional wellbeing programs and targeted interventions such as smoking cessation or parenting groups.
Strengths of the ACCHO model include:
Taking a holistic approach to people’s care – including considering multiple areas of a child’s life and factors that may influence their mental health and wellbeing
Having a ‘no wrong door’ approach, so when someone reaches out for support, they are never turned away without at least being linked in with the services they need
Providing warm referrals to services to reduce the burden on community members to navigate the complex service system on their own. This entails the service provider making contact with the provider or organisation on behalf of the child or family who are being referred, rather than just providing information.
Proposing a model of integrated child and family wellbeing services
We propose that this model could provide:
Information and evidence-based resources
Parenting programs for families and carers
Assessment and treatment planning for those referred by a primary care provider
Multidisciplinary team care for those with complex needs.
A multidisciplinary team would work together to support children and families with a variety of needs. The specific profile of these teams would be determined locally, but could include child and youth psychiatrists, paediatricians, psychologists, Aboriginal and Torres Strait Islander health workers or liaison officers, mental health nurses, occupational therapists, speech pathologists, physiotherapists and social workers.
This model would be physically implemented in multiple locations around the country, creating a network of skilled service providers. Teams would use a combination of face-to-face and telehealth approaches to maximise accessibility. This model enables culturally appropriate care via designated Aboriginal and/or Torres Strait Islander staffing or strong partnerships with local Aboriginal Community Controlled Health Organisations (ACCHOs). Relationships with local education providers (such as schools) and their mental health workforces would also be established to allow for holistic care and sharing of evidence-based resources.
This model would bring child development servicesl and child and family mental health services together. The needs of the child and family should drive genuine collaboration between service providers to provide effective care. While co-location of these services may facilitate this collaboration, co-location is not required to achieve integration. The holistic approach of this model mirrors that taken by ACCHOs and the Central Australian Aboriginal Congress.
Access
Children and families would be referred by a GP or another primary care clinician for assessment and treatment. Referral would not be dependent on a diagnosis, consistent with the wellbeing continuum approach. The referral process would be designed to be easy to access and not arduous.
The proposed model is not a walk-in centre model, however anyone entering would be connected with appropriate information and resources to ensure a ‘no wrong door’ approach. As per the action 1.2.d, staff would also be trained to identify parents and carers who are struggling with their own mental health and connect them with the necessary supports.
Funding
This model would require new funding. However, this model could emerge out of and extend current public health services as long as the funding was quarantined for working with children up to 12 years and their families.
In areas where there is a shortage of existing child mental health services or health services generally, establishing an integrated model would require additional funding for establishment. Local governance is an important feature of the model and could facilitate community engagement and collaboration with other local services.
Treatment
Services would be provided via a combination of face-to-face and telehealth approaches. In rural and remote areas and for families with limited financial resources, this needs to be accompanied by physical spaces in communities (such as community centres, GP clinics, or libraries) where telehealth services can be accessed with support. This is essential to mitigate barriers, including limited internet access or quality, affordability of internet enabled devices and unsuitable home environments.
Treatments that are more specialised (for example, interventions for highly traumatised children) would be provided in a limited number of locations. Because these locations would be networked across the country, those with specialised capabilities would undertake strategic planning and provide targeted:
Support for other locations or service providers (such as GPs) to directly help the child/family
Support for the child/family directly using face-to-face or telehealth approaches depending on the nature of the support to be provided.
The referral process between the locations with specialist services and those with more general services would be managed by staff, including outreach to families to ensure that there is continuity of care.
What would be the same at every location, and what would be locally tailored?
Standard
Multi-disciplinary service delivery with capability to support children up to age 12
Connected to other locations, as well as PHNs and LHDs
Access through referral
Ability to coordinate own and other services
Provide training and supervision opportunities
Undertake research and evaluation
Tailored
Level of funding required and local governance arrangements
Relationships with local community organisations (such as ACCHOs) and education settings
Exact services provided and staffing profile (connection with other locations will ensure all services can be accessed)
Way services are provided (for example predominantly face-to-face or virtual)
Why implement an integrated child and family care model?
Implementing the proposed model could address multiple objectives across this Strategy, including:
Providing supports directly to families (1.1)
Supporting place based approaches (1.3)
Improved system navigation (2.1)
Collaborative care (2.2)
Access and equity (2.3)
A system built for complexity (2.4)
A skilled workforce (2.5)
Collecting meaningful data (4.1)
Embedding evaluation and feedback (4.2).
The model ensures all families have access to quality, connected care that is easy to find and tailored to their local community, regardless of their child’s mental health and wellbeing level. It supports training and upskilling of the mental health workforce, and is an avenue for collecting data and feedback across Australia to continuously improve the services provided.
Actions 2.1
a. Build on and promote existing online navigational tools (such as HealthPathways) to enable both providers and community members to find the most appropriate locally available supports for children struggling with their mental health.
b. Review experience of transitions between services (including across jurisdictions and sectors) and redesign processes to ensure children and families experience optimal transition of care.
c. Establish model of integrated child and family care (see page 47-49) networked across Australia that provides holistic assessment and treatment for children 0-12 years old and their families.
d. Examine how policy, services and implementation affect transition from childhood to adulthood in the healthcare system, and redesign to allow for a seamless transition.
e. Model the current and future demand for mental health services and identify gaps.
Objective 2.2 Collaborative care
To effectively support a child’s mental health when they are struggling, a range of people are likely to be required to help, including medical professionals, allied health professionals, educators and families. Coordination between these groups is needed, to ensure all partners (including children, parents and carers) can agree on the plan for the child and know what their role is to deliver it.
While there is an acknowledgement of the need for better coordination and integration of services, it can be very challenging to put into practice at a policy, planning and service delivery level. There is often a lack of clarity as to exactly what integrated service delivery means, and what it is intended to achieve, with confusion about terminology so that coordination, collaboration and integration are often used interchangeably (see Box 6). There are also currently limited arrangements to enable a coordinated approach to care.
Box 6: Definitions of care coordination.
Care coordination has many labels, but all models and related concepts share common elements:
Numerous participants are typically involved in care coordination
Coordination is necessary when participants are dependent upon each other to carry out disparate activities in a child’s care
In order to carry out these activities in a coordinated way, each participant needs adequate knowledge about their own and others’ roles, and available resources
In order to manage all required care activities, participants rely on exchange of information
Integration of care activities has the goal of facilitating appropriate delivery of health care services.
The most frequently used terms are coordinated care, shared care, collaborative care and integrated care. Integrated care implies that care reflects the whole of a person’s physical and mental health needs, across providers in primary care, community and hospital settings. Collaborative, shared, or coordinated care is a model that relies on multiple service providers communicating about the child’s diagnosis and treatment, often via shared care plans led by a primary care provider.
Service delivery integration can occur at a number of levels. In the first instance professionals from different agencies and services can create informal networks – this type of collaboration might facilitate discussion about patients and shared planning of intervention and should be a bare minimum to expect of the service system. Then follow increasing levels of coordination and integration – more formal collaborative networks, common records, sharing of staff, more flexible governance arrangements, all the way through to true integration. At its optimal, this would involve co-location of a number of different services at the one site and include a shared vision with single governance arrangement and management. In addition, processes such as staff training, decisions about resources, record keeping, triage and assessment, and planning would all be integrated.
However, co-location of services does not always guarantee improved coordination. Agencies and services can operate from the same physical site and have minimal or no collaboration. Conversely there can be high levels of collaboration and coordination amongst services that are not co-located, though this type of ‘virtual integration’ poses particular challenges, especially if services are widely separated geographically. Co-location certainly does facilitate better linkages and improved collaboration between agencies and services.
While the focus of integration is usually on the system of services for children and families, it is unlikely that sustained and effective integration will occur without some sort of effort to improve coordination and collaboration at a policy and planning level. This is based on the premise that the wellbeing of children is beyond the responsibility of any single government department. Policy and planning need to be integrated across government portfolios, departments and agencies, and efforts made to coordinate federal and state resource allocation, programs and services. Results from such efforts in the past suggest that this will be an ongoing challenge.
The importance of collaborative care is highlighted for children with complex concerns who need to be seen by a number of agencies to get a good understanding of their issues. For example, Attention Deficit Hyperactivity Disorder (ADHD) and learning problems can co-occur but attention problems can also be a consequence of learning problems, as it is difficult to pay attention when you don’t understand what a teacher is talking about. To tease this out, both a psychologist and a child psychiatrist or paediatrician may sometimes need to see the child. Where a child has complex issues there may be numerous assessments needed (for example, psychology, psychiatry, speech pathology and occupational therapy). Currently, when these assessments are done in the private setting there is rarely someone available to draw all the information together for a child and their family.
Multidisciplinary case conferencing is one way of connecting all the people involved in a child’s care. It facilitates communication between the providers and gives an opportunity for the professionals, parents/carers and the child themselves to discuss what is needed and who is responsible for each component of care. Medicare funds case conferencing for people with chronic and complex care needs, as long as it involves a GP and at least two other health or community care providers (such as psychologists, social workers or speech pathologists). However, only the GP is able to claim payment for case conferencing, which means families must rely on the goodwill of the community care providers to participate ‘pro bono’ (action 2.2.a). For children and families with complex needs, care coordination is a critical ingredient of evidence-based care and should be funded appropriately (action 2.2.a).
As a central coordination point for the care of children, general practitioners play an important role in collaborative care. To ensure the GP is able to perform this role, any service (including services outside of the health system) that provides or arranges support for a child should be required to communicate their involvement to the GP (action 2.2.b).
Collaborative care also means involvement of parents and carers. Parents and carers want to understand how they can best support their child. Uncertainty about what they should do can lead to additional worry. Families may need guidance on how they should respond when their child is struggling, or how they can help create an environment that enables the child to flourish. This type of information could be provided by the service providers supporting the child. However, Better Access services (i.e. Medicare-funded) do not allow health professionals to claim (i.e. be paid) for consultations with parents without the child present. This limits the delivery of parenting strategies as a key or complementary part of a child’s treatment and recovery, as these conversations between a professional and a parent can be harmful if done with the child present. As a result, the current funding system creates barriers to parents accessing information from services that would in turn support their child (action 2.2.c).
Educators, non-government service providers and other community supports also report wanting a better understanding of how they can support a child when they are struggling with their mental health. However, mental health professionals are not required to provide feedback to educators or other service providers (other than a GP in some circumstances) despite the pivotal roles these people play in the child’s recovery. Feedback could be provided informally (phone call, email) or formally (inclusion as part of a care plan), but there are no consistent expectations or requirements that feedback is provided at all. Current barriers to mental health professionals providing feedback to other supports may include insufficient time, a lack of confidence in working with other sectors (such as educators) or a lack of confidence navigating the confidentiality boundaries (action 2.2.d).
Action is also needed to support the broader government service system (for example, police or community services) to refer children to support when they observe or engage with a child who may need assistance. Even adult-focused services can contribute to better supports for children. For example, services that help adults who are dependent on substances should be asking whether there are any children exposed to these issues, and then ensure those children are connected to relevant supports. As a minimum, reporting such things to a child’s GP, where possible, may ensure the child receives support and ongoing needs are monitored (action 2.2.b).
There is also a need for parental mental health care to be accessible via the same care pathways as for their children given the high concordance in mental illness across parents and children. A study investigating families with children attending mental health services reported that around 35% of parents had mental health issues themselves. This may be partly due to genetic factors – the heritability of mental illnesses is estimated to be between 40% and 80%, as well as shared environmental effects. Compared to children whose parents did not have mental health symptoms, children of parents who did report mental health struggles had significantly more severe symptoms at follow-up, indicating a vulnerability to poor outcomes for children in these families regardless of the child’s specific diagnosis.
Not only is it common for parents to struggle with mental health, but addressing parental mental illness is an important part of what child mental health services can do for children. It has been demonstrated that successfully treating maternal depression with medication will result in both lower rates of new diagnoses in children, and remission of the child’s own symptoms if they were struggling at their commencement of the parental intervention. This highlights the opportunity for improving child mental health at least partly through improving parent mental health – that is, treating a parent struggling with mental illness will benefit them and their child (action 2.2.e). Similarly, services supporting adults who have children should create an opportunity to connect the children with services, if required (action 2.2.f).
Currently, the care for mental illness in children and adults takes place in separate services, with public services inaccessible for parents and carers unless their mental illness is very severe. This means that for the majority of parents with anxiety or depression, treatment is limited to the private sector, which is often associated with significant out-of-pocket costs.
Given that families experiencing adverse circumstances (such as unemployment) are more likely to struggle with mental illness, many of these parents cannot afford to seek help and will forgo care, thereby worsening the parent’s and the child’s prognosis (action 2.2.g).
Improving the outcomes of these vulnerable families, starts with asking parents about their mental health when they present with their child to an outpatient service, and vice versa. This should include the siblings of the child presenting to services. Despite concerns from clinicians, data collections in outpatient clinics show that routinely asking parents about their own mental health is well accepted by parents. There is also an opportunity to use the almost universal setting of workplaces to support the mental health of parents. Where relevant, this should include programs that incorporate strategies for new parents, especially in the early weeks and months of adjusting to parenting, and during the return to work phase (action 2.2.g).
Things we can build on
In some states and territories early childhood learning services (known as ‘children’s centres’ and ‘child and family centres’) provide a range of services across care, education, health, community development activities and family services, tailored to local needs. This includes regular and occasional care for babies, toddlers and children in the year before school, as well as playgroups, and parenting programs. In some cases, antenatal services are also available, and there is an allied health program (delivered by speech pathologists and occupational therapists) that builds capacity of centre staff and parents in identifying children from birth to 3 years who are at risk of developmental delay. Centres also have family practitioners who can support vulnerable families and children, including those struggling with issues of domestic and family violence, drug and alcohol use and mental illness. In an evaluation of these services, parents reported that the children’s centres had positive impacts on their wellbeing, parenting capacity and parenting practices.
The Families as First Teachers (FaFT) program is an early childhood and family support initiative for remote Indigenous communities across the Northern Territory. The program, delivered in schools by the Northern Territory’s Department of Education, provides early learning playgroups and parenting programs on child development and health to enhance children’s early learning and prepare children for successful entry to school. Early childhood professionals, and local Indigenous family liaison officers and playgroup leaders, deliver the programs to families. This approach has been evaluated in terms of impact on children’s language acquisition and general development, with strongest results seen in children who had the highest participation levels. In addition, the embedding of culture and local language was an essential component of its success, along with quality and fidelity of program implementation.
Actions 2.2
a. Incentivise all relevant service providers to participate in case conferencing. This could be done by enabling providers of all disciplines to claim the existing case conferencing Medicare item numbers.
b. Require all service providers, including outside of the health system, to communicate with a child’s nominated GP about supports they are arranging or providing. This communication should be regular to ensure the GP is aware of any changes in the supports a child is receiving.
c. Enable service providers to claim Medicare payments for consultations with parents and carers as part of a child’s mental health treatment, removing the requirement for the child to be present.
d. Require mental health professionals to communicate with educators and other service providers about a child’s treatment and support plan, with the family’s permission and subject to this being deemed clinically appropriate.
e. Equip child mental health services to identify parents and carers who are struggling with their own mental health and require them to connect those parents and carers with appropriate supports.
f. Equip adult mental health services to identify any children in their clients’ care who need mental health support and require them to connect those children with appropriate supports.
g. Include content specifically targeting parents in workplace mental health programs, with a particular focus on new parents during the return to work phase.
Objective 2.3 Access and equity
Many children and families are unable to access timely treatment. A long delay in children accessing supports can have a negative impact on the child’s outcomes and is contrary to the principles of prevention and early intervention. Problems accessing services could be due to a range of reasons, including high out-of-pocket costs, long waiting lists, some services requiring a diagnosis to access treatment, or unintentionally high severity thresholds simply due to difficulty meeting demand.
The mental health system generally comprises public services, private services, and some non-government services. Public services are provided at no cost to families, they are typically designed to cater for children in complex circumstances, but they often have long waitlists and/or high severity thresholds to access a service. Private services are associated with (sometimes high) out-of-pocket expenses, are not designed to manage complex cases, and they can also have long waitlists. Non-government services often provide specific programs for particular cohorts of children and/or families, which can mean many don’t meet criteria for access because of factors such as geographic boundary limits, specific diagnosis (or lack thereof), or age.
Out-of-pocket costs mean that an individual service is either ineligible or only partially covered by a relevant Medicare item. Out-of-pocket costs for Australians seeking mental health services are known to be relatively high, and people with chronic conditions are more likely to forego care because of the associated costs. Adults with depression, anxiety and other mental health conditions are seven times more likely to forego care due to cost compared to people with no health condition (action 2.3.h).
For many families, the cost of private services is prohibitive, but they do not meet severity thresholds to access the free public services. There is a lack of capacity within public mental health services for those who currently need them. CAMHS must triage based on severity and a lack of capacity results in services being directed to older children and adolescents with acute (i.e. crisis) presentations. This makes it difficult for families to identify an affordable alternative service for a child with lower level needs. Children are often also placed on long waitlists to access publicly funded paediatric services, with some children turned away when services have no capacity (action 2.3.a). Being placed on waitlists and turned away from services can be incredibly disheartening for children and families, as well as being detrimental to their mental health and recovery. This can leave children in limbo, delaying or preventing access to the supports they require.
Access to mental health care can also be improved by having the onus on the service system (not just families) to make space for conversations about children’s mental health and offer supported access to services. Service providers should make the most of (often incidental) opportunities to ask parents directly if they have concerns about their child’s behaviour or development. Increased training and additional professional support for GPs and paediatricians on how to best help families and children who are struggling could result in a more efficient way to provide these families with the support they need. This would help them be more competent and confident in providing interim responses and enabling care planning processes to occur (action 2.3.b). Similarly, services that work with children experiencing difficulties with language, learning or other aspects of development provide an opportunity to discuss any concerns about mental health and connect with services where appropriate.
Face-to-face services are generally the preferred service delivery model – this approach is familiar for most people and it enables building of rapport with health professionals. However, access to face-to-face services is not possible for everyone, especially for families living in regional and remote areas where there may be no professionals with the required skills in child mental health. To access services, children and parents may need to travel long distances at their own cost, and at the expense of missing school or work and spending time away from the rest of their family and community (action 2.3.c).
One approach to support increased face-to-face care, is to equip primary care services with the appropriate resourcing and training, so that they have sufficient capacity and expertise to support child mental health locally. By increasing the ability of primary care to support children who are struggling with less acute but more common difficulties, referrals to specialist services can be reduced and equity and accessibility for those outside metropolitan areas is likely to be increased.
Australian governments also provide some incentives for health professionals to work in regional and remote areas (for example, the Workforce Incentive Program), but incentives typically have strict accessibility criteria and may not cover mental health services. Incentives, such as subsidised study or training, professional support and renumeration adjustments, should continue to be explored to increase workforce supply in these areas and reduce the service gap for communities by increasing both accessibility and affordability.
Telehealth services are also an important adjunct to face-to-face service delivery. However, there are currently restrictions on who can access telehealth services (i.e. specific postcodes) and which professionals can deliver services (for example, nurse practitioners cannot access Medicare-funded telehealth items). Given the success of this measure during the COVID-19 pandemic, it is an optimal time to continue to build expertise in delivering telehealth services effectively, as well as expanding their availability. There is growing confidence between service providers and service users with this modality of care, and a recent senate committee recommended that telehealth items introduced during the pandemic become permanent (action 2.3.d). Telehealth should also be utilised to support primary care providers and those who are more geographically isolated through activities such as supervision, professional advice and shared care.
Many services also lack cultural accessibility in that they are not acceptable or appropriate for children and families who do not identify with the dominant culture. This may include those from culturally and linguistically diverse communities and Aboriginal and Torres Strait Islander communities. Barriers can be both cultural and structural, including discomfort with the physical environment of the service or a lack of literacy about how health services typically operate (such as appointments, payments, referrals, roles of different providers and overlapping interventions). Information about health services should be available in multiple languages. In 2016, half of Australia’s humanitarian intake (51%) were aged less than 25, and 28% were under 12 years of age. Children who come from culturally and linguistically diverse communities may be at higher risk of facing mental health challenges. Despite being at higher risk, children from these communities often face barriers when seeking help. The Australian Refugee Health Practice Guide suggests including mental health assessment in a comprehensive health assessment upon arrival to Australia, ideally within one month of arrival. Children under 11 years of age are currently offered less immigration medical screening compared to adolescents and adults, which lessens the amount of contact with a GP.
Mental health practitioners must ensure their services are culturally appropriate. Psychiatrists in the private sector can access the Translating Interpreting Service (TIS) for free if they are providing services that can be claimed back through Medicare rebate. All mental health services should be aware of how mental health is conceptualised in different cultures. Incorrect assumptions can lead to unrealistic expectations about the extent to which people will be knowledgeable about medical care models and styles of engagement. To avoid these pitfalls, it is crucial that services be designed, delivered and evaluated with significant involvement from the people who are the intended users of the services (actions 2.3.e and 2.3.f). Aboriginal and Torres Strait Islander children and their families should be able to access support through ACCHOs. Where only mainstream services are available, they will need to undertake measures to ensure cultural safety of the service.
More broadly, it is crucial that services be designed in a way that makes children and families feel safe and comfortable. Children and families are not commonly involved in the co-design of services, which means they miss out on opportunities to contribute to developing services that are inviting and acceptable to them. Young people report experiences of services not always understanding their perspectives – for example, the purpose and function of therapy is not always explained in a way that makes children feel safe to openly share their innermost thoughts and feelings. Children may not be given a choice about how they can engage with services (for example, non-verbal activities as well as talking), or they might feel that they are not given enough opportunity to build trust with a professional before being expected to engage (action 2.3.e).
Things we can build on
Many families have benefited from access to telehealth services, with the use and acceptance of these services increasing during the COVID-19 pandemic. Telehealth services have been used in rural and remote areas for some time now. A recent systematic review found that patients and caregivers were generally satisfied with telehealth services, including in the domains of system experience, information sharing and consumer focus. Even young children have been able to access services successfully through this model (see Box 7). While telehealth services are not the optimal solution for all families, they can play a useful role increasing the accessibility of professional services and advice for those whose access to local professionals may be limited.
The NSW Child and Adolescent Psychological Telemedicine Outreach Services (CAPTOS) has been in operation since 1996. The function of the service is to provide psychological and psychiatric advice on assessment and treatment of children in rural areas to local clinicians.
It also serves to support clinical education and supervision for non-specialist rural clinicians. Under this model funding is controlled by the rural provider rather than centrally by the specialist service (action 2.3.g). An initial evaluation focused on user satisfaction found that 95% of rural families and clinicians using the service were highly satisfied, and subsequently further services including telenursing, professional skills development, sabbaticals for rural clinicians and clinical skills workshops were developed.
In NSW, a consortium of PHNs have jointly commissioned the GP Psychiatry Support Line 2020. The service is staffed by psychiatrists and is available free to GPs practicing within the associated PHN regions. It has been active since 2019, and can assist with diagnosis, investigation, medication and safety plans to help GPs manage the care of consumers in the community (action 2.3.b).
Box 7: Telehealth services
Mia’s* 4-year-old son struggles with anxiety and regularly sees a psychologist along with other health professionals, such as a speech pathologist. When the COVID-19 pandemic prevented her son from being able to see his psychologist in person, they were given the option of consultations through telehealth services. Given how young her son was she was unsure how well he would engage. However, she found it to be more effective than anticipated. Her son was happy to sit at the computer and engage with his psychologist as well as other health professionals.
Mia found that receiving services through this model also had additional benefits that she had not foreseen. She reported that by being able to receive the services at home, this reduced the time and stress of travelling to and from appointments. It also resulted in the opportunity for his psychologist and teacher to meet via video call and discuss opportunities to support her son. She felt that this had enabled her son to receive more integrated care without significantly increasing the costs for their family.
*Name has been changed to protect anonymity
Actions 2.3
a. Increase resourcing for public mental health services to support children aged 12 and under. Funding should be attached to implementation of the model of integrated child and family wellbeing services (action 2.1.c).
b. Provide accessible and affordable training and resources to GPs, paediatricians and other care providers to help them respond to children and families who are struggling, including for practitioners in regional and remote areas.
c. Implement innovative service delivery models that integrate face-to-face and telehealth consultations, digital interventions, and phone helplines to improve access to services.
d. Commit to ongoing Medicare funding for telehealth services.
e. Embed the principles of genuine co-design into the design, delivery and evaluation of all services supporting children and families; actively inviting involvement from the people the service aims to support.
f. Establish accountability mechanisms (for example, audit and public reporting) that encourage services to improve their accessibility for children and families, including those from Aboriginal and Torres Strait Islander communities and culturally and linguistically diverse communities.
g. For programs involving specialists providing advice, education or professional support to rural providers, adopt governance arrangements that make funding dependent on the rural provider’s needs being met.
h. Ensure free or low cost mental health services are accessible to parents and carers with mental illness.
Objective 2.4 Built for complexity
Both health and social services (such as child protection) have a role in ensuring that children and families dealing with complexity are well supported. This may include where children have intellectual or developmental delay, children whose parents have struggled with their own mental health, children who have experienced or at-risk of entering the child protection system, and families that have faced significant trauma and adversity. These children and families may be more likely to require support from multiple services, which may include specialised expertise. Children and families with complex needs would benefit from a nominated care coordinator (action 2.4.a). This role would support families to navigate the service system, and to liaise with the clinicians and educators involved in a child’s care. Care coordination should be offered to families at multiple points of contact with the service system including the initial referral, during treatment and at any review points.
Where there are systemic or structural barriers preventing children and families accessing the right systems and support (see Box 2), links need to be strengthened between existing community based touchpoints and general health services. For example, specific postnatal pathways for parents from refugee backgrounds (and other new migrants) linking them with enhanced maternal and child health services and offering parent groups to second and subsequent children for at risk families. Other avenues include specialised refugee and asylum seeker health services, General Practitioners, torture and trauma services and settlement services who may also provide expertise and pathways that would facilitate connection with appropriate services.
Children at risk of suicide require targeted services and supports. While this Strategy focuses on prevention, it is vital that there are pathways for treatment when children are in crisis. In 2019, 96 deaths by suicide occurred among children and adolescents (aged 5–17) with the majority occurring in those aged 15–17 (80% in 2019). From 2008-9 to 2018-19, the rate of intentional self-harm hospitalisations in females aged 14 and below doubled. Suicide prevention programs and activities, such as aftercare, must consider the unique needs of children who may access the services (action 2.4.b).
A specific group of children with the most complex needs are children under the care of the State, including those in contact with the justice system. These children are likely to have been exposed to trauma that has led them to enter State care and are also at risk of experiencing trauma within the system.
Children who have experienced the child protection system are twice as likely to experience mental illness, and children who have experienced out-of-home care are five times more likely. Higher rates of mental illness are also observed in children who have experienced youth detention. There are also children who are at-risk of entering care of the State. Under Australian law, mandated reporters must notify authorities of suspected child abuse or neglect. Mandated reporters vary between states and territories, but generally include teachers, early childhood education and care practitioners, doctors, nurses and police. Children who are the subject of notifications to authorities are also likely to be experiencing significant trauma.
These children are likely to benefit the most from high-quality, well-coordinated mental health supports. Currently, these children are more likely to be turned away from services than other children as their needs can be more complex, and services report that they do not have the capacity to cater for them. This can mean that children in State care, or who are at high-risk of requiring care services, are unable to access health and wellbeing support until their mental health has declined severely. Therefore, children under the care of the State, as well as those who have been the subject of notifications, need to be supported more frequently and as a priority in order for any mental health strategy to have maximum impact (action 2.4.c). This includes children who have been placed with extended kin or community networks under the Aboriginal and Torres Strait Islander Child Placement Principle, which aims to keep children connected to their families, communities, cultures and country and to ensure participation of Aboriginal and Torres Strait Islander people in decisions about their children’s care and protection.
Box 8. Trauma-informed care
Trauma-informed care is an approach that involves understanding individual experiences of trauma, and recognising the consequences of a history of trauma. Trauma-informed care can be utilised in any profession that provides care to another person, and allows care to be more accessible to people with a history of trauma. Trauma-informed care is guided by 5 key principles: trauma awareness and acknowledgment; safety and trustworthiness; choice, control and collaboration; strengths-based and skills-building care; and cultural, historical and gender issues awareness.
Trauma awareness and acknowledgement involves bearing witness to a person’s history of trauma, and acknowledging the ongoing effects the trauma has on their life. It is not necessary for trauma to be explored explicitly, but a general overview is beneficial for care providers. It is important to acknowledge and validate the shame that can be caused by a history of trauma.
Safety and trustworthiness involves making a person feel that they are safe, and recognising the need for them to be provided with physical and emotional safety. It is beneficial for the procedure of care to be consistent and predictable. People with a history of trauma will also benefit from feeling physically and emotionally safe in the environment where they are receiving care.
Choice, control, and collaboration involves actively engaging a person in the care process. People with a history of trauma will benefit by being provided with multiple choices for their care. Choices may be as simple as allowing the person to choose whether they engage with, or do not engage with care. Providing choices allows people with a history of trauma to have a more active engagement in the care they are receiving, and can reduce passivity towards care.
Strengths-based and skills-building care involves highlighting a person’s strength and resilience. By highlighting the individual strengths of a person, the person who is receiving care will be encouraged to view themselves more positively and may become more willing to work through their trauma.
Cultural, historical and gender issues awareness involves being informed about issues related to a person’s culture, ethnicity, and social identity. Having an awareness of issues that relate to a person’s personal identity can allow care providers to provide more sensitive care. People with a history of trauma will benefit from care providers who are sensitive to group-marginalisation, and who understand the ongoing effects of trauma experienced by marginalised groups.
Trauma-informed care can be especially beneficial when working with Aboriginal and Torres Strait Islander families. Care providers who work with Aboriginal and Torres Strait Islander families should be educated about historical trauma, trauma symptoms, and impacts of trauma. Education around historical trauma can include the forced separation of Aboriginal children from their families and assimilation policy. Education around trauma symptoms can examine symptoms such as substance misuse, poor self-regulation, and psychosomatic illness. Education around the impacts of trauma can explore mistrust towards government workers, fear reactions, and wellbeing outcomes. Understanding the history of trauma Aboriginal and Torres Strait Islander families have faced will inform more appropriate engagement strategies, prevent families being re-traumatised and allow care providers to be more compassionate.
Governments have an increased responsibility to serve this population of children who are directly under their care. While child protection systems are focused on making sure the child is safe, this is not enough. Children in out-of-home care remain at very high risk for a range of health, developmental and mental health problems over the long term. International models use the term ‘corporate parent’ to describe the additional responsibility that governments have for looking after the health and wellbeing of children in out-of-home care. Given the range of difficulties these children often face, all government portfolios should play a role in supporting them and improving their wellbeing (action 2.4.d), not just those with explicit responsibility for child protection. It should also be noted that prioritisation of children in care is not intended to override clinical triage, but rather the child’s care environment should be taken into consideration as part of this process.
Children with a disability or a chronic illness are at significantly higher risk of having mental health issues than children without a disability. Those with an intellectual disability are up to four times more likely to have a diagnosable mental illness. In addition to the disability itself, the mental illness has an impact on school participation, relationships, family functioning and long term outlook, as the mental health problems may persist throughout the life course. The combination of disability and chronic illness places these children at particular risk, with studies finding an approximate doubling of risk of mental illness for children with chronic health conditions, and these are likely to persist into adolescence. Furthermore, there are indications that anxiety symptoms can worsen the outcomes of physical illnesses (action 2.4.e). Given the significant relationship between physical and mental health, children struggling with their mental health should also be examined for physical health problems to ensure a holistic approach to health and wellbeing (action 2.4.f).
This increase in risk for children with disability has implications for the way that the National Disability Insurance Scheme (NDIS) is structured and functions, and all disability services need to be aware of and address the likelihood of and potential for associated mental illness. At present, the NDIS has an Early Childhood Early Intervention approach which supports children aged under 7 years who have a developmental delay or disability and their families and carers. This approach is administered by an Early Childhood Partner who develops a plan for each child including referral to local supports.
The National Roundtable on Mental Health of people with intellectual disability recommended development of greater workforce knowledge and skills in prevention and timely intervention for those who need mental health support. For children, this may include community led interventions, such as whole of school approach to creating an inclusive culture, or more targeted interventions such as opportunities for students to practice complex social skills in stepwise fashion. Within health and social services, there are barriers such as lack of investment and research into mental health assessment tools and effective treatment approaches for this population, along with insufficient (and under-funding of) specialist services that offer expertise in both mental health and intellectual disability (action 2.4.e).
Similar challenges exist for children with neurodevelopmental disordersm, with increasing access issues for children requiring a complex autism assessment by a multidisciplinary team. It is estimated that 1-2.5% of Australian children experience some form of Autism Spectrum Disorder (ASD). Families of children with ASD experience higher rates of mental health struggles, and children with undiagnosed or poorly treated ASD often become increasingly anxious and depressed with age.
The Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability noted that Aboriginal and Torres Strait Islander people with disability are especially vulnerable to violence, abuse, neglect and exploitation, with additional risk factors including significant collective trauma, poorer health, more frequent contact with the criminal justice and child protection systems and experiences of systemic discrimination. While ACCHOs are skilled at adapting and designing services to meet the often complex needs of their specific communities, available funding structures do not always support these services to be delivered in the way the community would like. Mainstream funding frameworks can be rigid and require demonstration of specific outputs (for example, number of 50-minute therapy sessions) that may not be relevant to the nature of the service model the community requires (action 2.4.g). In addition, mainstream mental health services may not have a sufficient understanding of how Aboriginal people identify with disability and the role of culture within these beliefs. Disability is a western concept, with many Aboriginal languages and cultures having no equivalent word or concept. Traditionally, disability is seen as an integrated part of the person, unique to the individual and embraced as part of their social and emotional wellbeing. It should be recognised that Aboriginal and Torres Strait Islander people with disability experience intersectional disadvantage, inclusive of ableism and racism, as well as resultant poorer outcomes and service access.
Systems and criteria that prevent children with complex needs from accessing services should be redeveloped to ensure that the children who are in most need of support are not turned away due to a lack of capacity or capability (action 2.4.h).
Things we can build on
The National Standards for out-of-home care require that children and young people have their physical, developmental, psychosocial and mental health needs assessed and attended to in a timely way. This means that the child or young person’s needs are identified in a preliminary health check upon entering care, in order to receive specialised services. The National Clinical Assessment Framework for Children and Young People in out-of-home care supports the implementation of the National Standards. The Framework provides age appropriate (less than 1, 1-5 years, 6-11 years) assessment elements, including measures across cognitive and language development, behavioural and emotional development, mental and physical health and health history. In the area of youth justice, the Youth on Track scheme in NSW has been effective in supporting children aged 10-17 years who are at risk of becoming entrenched in the juvenile justice system. The program involves providing targeted support for children and families, including family interventions, behavioural interventions and strategies for engaging children with education. Children and families may be referred to this program through schools or by police (action 2.4.i). Elements of the program which were found to be particularly effective included the focus on early intervention, the holistic and tailored approach (including working with families), the trained and skilled professionals, and collaboration with other services. The program has been found to contribute to positive attitudinal and behavioural changes in young people referred to the scheme, as well as changes in lifestyle to reduce the risk of offending amongst the youth, such as enrolling in vocational training and developing new friendships or community connections. A version of the scheme ‘Getting on Track in Time – Got It!’ targeting younger children (aged 5-8) displaying behavioural concerns and conduct problems is also delivered in NSW schools.
Actions 2.4
a. Provide specific funding for care coordination to be available to children and families with complex needs, offered at key points of contact with services.
b. Suicide prevention programs and activities, such as aftercare, should consider the unique needs of children who may access the services.
c. Require relevant services to give priority access to children who are in State care, or who have been the subject of notifications, and Aboriginal and Torres Strait Islander children who have been placed with kin/community networks, and for care to be provided more frequently.
d. Require all government departments to outline and regularly report on what they do to support children in State care, with independent monitoring of outcomes.
e. Require relevant services to outline and regularly report on what they do to ensure they are accessible and effective for children with physical or intellectual disability or neurodevelopment disorders, with independent monitoring of outcomes.
f. Children struggling with their mental health should also be examined for physical health problems to ensure a holistic approach to health and wellbeing.
g. Child and family mental health and wellbeing supports for Aboriginal and Torres Strait Islander communities should be delivered by Aboriginal Community Controlled Organisations wherever possible, with activity and outcome measures to be collaboratively determined between the funder, service provider and the community to ensure they are appropriate.
h. Redevelop systems and criteria that prevent children with complex needs from accessing services, including addressing workforce capability where required.
i. Build on holistic support models for children who have had contact with the justice system or are at risk of coming into contact with the justice system.
Objective 2.5 Skilled workforce
Staff working across primary care, non-government services, the private sector, and public mental health come from a wide range of disciplines and training backgrounds. As a result, the quality of care children and families receive is variable. This is unacceptable – the quality of care a child or family receives should not depend on which staff member they happen to see.
Child and family mental health is considered an area of specialty that receives minimal attention in the majority of training courses and there are limited opportunities to gain expertise in child mental health through on-the-job training (actions 2.5.a and 2.5.b). More support for training in this area needs to be explored for both vocationally and university educated professionals, including early childhood educators (objective 3.3) and health providers. There is also a shortage of publicly funded positions for a range of health disciplines, which has flow-on effects to training capacity in the public system and inadvertently encourages graduates to directly enter the private system. This limits opportunity to build child and families expertise in public (i.e. free or low-cost) service settings (action 2.5.c).
As for many other health services, there is a dearth of mental health professionals for children in rural and remote areas. The provision of training and education for child mental health professionals is largely only available in metropolitan areas. Supports for rural mental health professionals (training, workforce and pastoral) are lacking, adding to the burden experienced by professionals who are located remotely. Market failure in rural and remote areas also results in private practitioners being drawn into larger metropolitan areas, diminishing the supply of desperately needed child mental health professionals in more remote communities (action 2.5.d).
These issues highlight the need to engage with existing health professionals already anchored to rural and remote areas, to promote development of their education and skills, and demonstrate career pathways from graduation to retirement (action 2.5.b).
For those who work in the public health system, consistently dealing with more complex ‘crisis’ cases can result in clinician burn-out and subsequent staff turnover. As a result, services often find that senior practitioners move to the private sector where they can work with a more varied mix of clients. While a number of system reforms are required to address these issues, a key focus of this Strategy is to deliver better interventions, earlier. It is anticipated that this would in turn reduce the unrelenting demand on public mental health services and enable them to provide earlier interventions.
A skilled mental health workforce is also one that has strong cultural competence, with research indicating that the therapeutic alliance is strengthened when practitioners have positive constructions about culturally and linguistically diverse clients, and have been exposed to clinical experience with culturally diverse clients, and discussion of multicultural counselling issues in supervision as part of their training. Lack of Indigenous health workers in services leads to underuse of services, while increased cultural understanding and culturally responsive service delivery increases access and frequency of visits (action 2.5.e). The young age profile of Australia’s Aboriginal and Torres Strait Islander populations may also have workforce implications that affect service delivery. In addition, financial support for ACCHO workers may be crucial to support their participation in education and training, given low salaries and community expectations of shared resources.
Finally, a skilled workforce is also one where dedicated researchers are well-integrated, if not embedded directly within clinical service provision. These roles need to be seen as just as important as their clinical counterparts and they need to be accessible and attuned to the specific research needs of the provider, as well as able to liaise with researchers outside the organisation when required. Services also need to be provided with funding for and access to data capture and reporting systems that are easy to use.
Things we can build on
In some cases, rural training pathways that include an element of focus on mental health already exist. For example, all Fellows of the Australian College of Rural and Remote Medicine undertake one year of Advanced Specialist Training as part of their core training. They can elect which discipline they spend their Advanced year on, with mental health and paediatrics as one option. However, unlike for some specialisations (such as obstetrics or anaesthesia), professionals with additional mental health specialisations are not remunerated for these advanced skills. This currently acts as a deterrent to professionals taking the mental health pathway (action 2.5.b).
The Extension for Community Healthcare Outcomes (ECHO) model has been used to effectively build the capacity of primary care clinicians to manage complex health issues in areas where there may be an absence of specialist expertise. In this model, professionals meet on an ongoing basis through telehealth platforms to enable specialists to share knowledge and advice with primary care clinicians in local communities. Use of the ECHO model for providing mental health management in primary care has been found to increase knowledge and self-efficacy and reduce feelings of professional isolations amongst rural health professionals. This is particularly important in rural areas, where ongoing supervision or professional support is often lacking.
Communities of practice is another a model for sharing ideas, insights and strategies between professionals with involvement, interest, or concerns in a particular area of practice. These communities bring together professionals from different disciplines and organisations and have been used in the healthcare sector to help change and improve practice (action 2.5.f).
The Royal Far West model of rural and remote program and service delivery for children offers multidisciplinary care both face-to-face and via video conferencing. They offer paediatrics, psychiatry, psychology, speech therapy, occupational therapy and social work services, and over half of their services are already delivered by telecare as part of their paediatric developmental program. If attending face-to-face, children and their families attend a free week-long residential program that comprises assessment, diagnosis, review and treatment. Continued schooling is available on site for children and their siblings, with technology-based outreach learning and literacy programs available for ‘telecare’ program participants.
Professional training and development are being offered through the Emerging Minds: National Workforce Centre for Child Mental Health project. The project aims to build the capacity of organisations and professionals who work with children (0-12 years) and families to identify, assess and support children at risk of mental health difficulties. Courses are free and available online, targeted at professionals in health, social or community services. Courses are staggered in their complexity from introductory modules through to evidence-based practice courses which teach hands on skills.
The National Mental Health Service Planning Framework - Planning Support Tool, is a population based planning model that provides resource estimates to guide mental health service planning. The tool allows users to estimate the needed and expected demand for mental health care and the level and mix of mental health services required for a given population. This in turn should guide the relevant local workforce projections (action 2.5.g). PHNs are also critical as part of local planning and commissioning.
Actions 2.5
a. Increase requirements for early career training in child and family mental health for all relevant service providers.
b. Incentivise existing service providers (including GPs, maternal child and family health nurses and allied health), with a focus on practitioners in rural and remote areas, to complete training in children and family mental health assessment and treatment.
c. Support public mental health services to act as training facilities for new graduates through designated training places and funding of supervision time.
d. Create and incentivise training opportunities for mental health professionals (for example, psychologists, psychiatrists, social workers, nurse practitioners) to work in regional and remote areas.
e. Develop cultural understanding amongst health professionals to work safely and effectively with Aboriginal and Torres Strait Islanders children and families, and provide greater support for Aboriginal Health Workers to engage in child mental health focused ongoing education and training.
f. Build on existing models of supervision and case consultation for private practitioners using a peer support/supervision model.
g. Develop workforce projections in the public sector based on evidence and epidemiology and use these to inform further recommendations.
The below table outlines some proposed indicators of change. If the objectives of this focus area are realised, we would expect to see improvements in the below.
Focus Area 2: The Service System – indicators of change
2.1. Uptake of integrated care models and changes in system cohesion
2.2. Uptake of child mental health and wellbeing services
2.3. Changes to the MBS and rates of use
2.4. Targeted investment in the mental health and wellbeing of priority populations
2.5. Uptake of training and professional development in child mental health and wellbeing
Last updated:
Acknowledgement of Country
The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the lands and waters on which we live, work and learn.
Diversity
The Commission is committed to embracing diversity and eliminating all forms of discrimination in the provision of health services. The Commission welcomes all people irrespective of ethnicity, lifestyle choice, faith, sexual orientation and gender identity.
Lived Experience
We acknowledge the individual and collective contributions of those with a lived and living experience of mental ill-health and suicide, and those who love, have loved and care for them. Each person’s journey is unique and a valued contribution to Australia’s commitment to mental health suicide prevention systems reform.