The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the
lands and waters on which we live, work and learn.
Aboriginal and Torres Strait Islander peoples should be aware that this website contains images or names of people who have passed away
The National Children’s Mental Health and Wellbeing Strategy Report
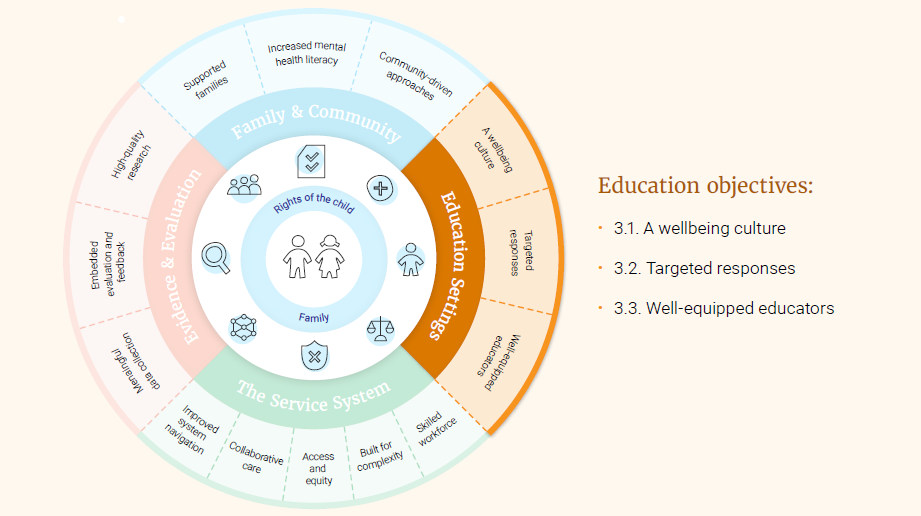
Focus area 3: Education Settings
This section outlines key issues and recommendations in relation to supporting mental health in the education context, which for the purposes of this Strategy, includes early childhood learning services and primary schools. All educators and education settings have a role to play to promote child mental health and wellbeing, including where a child and family has complex needs. The Commission recognises that education settings are already doing a considerable amount to support the wellbeing of children. The actions outlined below aim to build on this, with an emphasis on supporting educators in this role, not creating added burden.
Within the education sector, supporting children’s mental health and wellbeing needs to be central to the frameworks and standards on which the education and early childhood systems are built. Key objectives in this focus area include creating a wellbeing culture, planning for mental health and wellbeing, and engaging, supporting and equipping educators.
Why the educational context is so important.
Education settings provide an ideal environment to build resilience, support and empower parents and carers, and identify and intervene early in emerging mental health issues. Especially because they are a relatively universal, nonstigmatising environment where children can be observed for long periods in multiple contexts.
Education settings are already providing support in many cases. Data from the Young Minds Matter survey (the second Australian Child and Adolescent Survey of Mental Health and Wellbeing) indicate that teachers and other staff provide nearly 20% of students with informal support for behavioural and emotional problems, with staff members suggesting that additional help was needed in around 40% of cases. In addition, 11.5% of students have used a school-based service for support in the last 12 months, with 22.6% who used a health service having been referred by the school.
Consideration of early childhood education is an important aspect of this Strategy given there are lifelong benefits of early childhood education to individual children and families. Early childhood education helps children’s cognitive, social and emotional development, with greatest benefits for vulnerable or disadvantaged children. Quality early childhood education can help reduce the chances of these children being left behind, with flow on effects on learning and academic progress, school completion, and employment and income outcomes. Quality early childhood education also has long term economic benefits through increased productivity and reduced need for spending on remedial education, justice and health services. There are also immediate economic benefits from parents, particularly mothers, being able to increase their participation in the workforce. One Australian report found that the return on investment of offering universal early childhood education was 103%.
Objective 3.1 A wellbeing culture
Educational settings provide a unique and almost universal opportunity for promoting child mental health and wellbeing with 90% of eligible children enrolled in a pre-school program the year before full time school, and attendance rates of at least 90% in the primary school years. Given this opportunity, it is imperative that all educational settings play their role in promoting mental health and wellbeing in their students. For children and families who are not engaged with schooling, alternative strategies are needed (objective 1.1).
Children spend large proportions of their days in the classroom and the playground, and it is where much of their social interaction with peers occurs. However, there is currently wide variation between schools and early childhood learning services in the culture around mental health. Schools vary in terms of how regularly mental health is spoken about, how accepted and easy it is to access support, and educators’ awareness and understanding of mental health. Schools provide opportunities to discuss trusting relationships, kindness, respect, managing challenges and bouncing back, and how to look after mental health with good food, sleep, activities and hobbies. Schools could address these issues, as well as the challenges of the digital environment and screens, more systematically and consistently.
Some schools and early childhood services have policies and procedures that contribute to stigma and a negative culture around mental health. For example, young people report feeling ‘marked out’ for accessing support services through their school. This was because the process by which students were referred to or accessed supports was not managed discretely, and the students lacked control in the process. Children and young people reported that this made many feel uncomfortable to seek help in the school environment (see Box 9). Policies and procedures should be reviewed to address potentially stigmatising elements (action 3.1.a).
Box 9: Differing approaches to mental health and wellbeing in schools
Annie* reported having two very different experiences with mental health and wellbeing support at the two schools she had attended.
She explained that at her primary school, she had not realised that they had counselling services available for most of the time she was at the school and that mental health had generally not been talked about. She reported that it was only once she started being severely bullied that she was directed to the school counsellor. Annie reported that when the counsellor wanted to have a session with her, the counsellor would walk into the classroom and ask Annie in front of the whole class which made her uncomfortable and embarrassed.
Annie reported a very different experience at her new school. She explained that there was a mental health team at the school that the students all knew about and it was made clear there was a welfare counsellor they could see if needed. She reported that mental health was something that was spoken about throughout the school, including at school assemblies. Discussing mental health was normalised and students would encourage each other to seek help and speak to the counsellor if they were struggling. Annie reported that the teachers were also proactive at checking in with students and asking if they were okay when they were looking upset.
* Name has been changed to protect anonymity
Educators, particularly in school settings, are working within a busy curriculum, and mental health and wellbeing competes against a number of different public health areas for space and attention. Some schools have wellbeing teams, school nurses, chaplains or other staff who have a dedicated role in supporting children’s wellbeing. However, there are not always dedicated staff to progress mental health and wellbeing initiatives and to ensure that the early childhood service (action 3.1.b) or school (action 3.1.c) is providing the best possible support for students.
The way education settings approach mental health and wellbeing contributes significantly to whether children access supports when needed. Both children and families describe wanting education settings to cultivate open and supportive conversations about mental health and wellbeing so that peers can encourage each other to seek support if they notice a friend struggling. This may be achieved using formal and informal opportunities such as through assemblies, awareness days, or student projects/activities (action 3.1.d).
Proactive promotion of resources and supports to children and families is also key, including those available through the school, as well as external options. This could be achieved through orientation processes, assemblies, newsletters, or dedicated information sessions (action 3.1.e). Schools are also an important avenue for enabling migrant, refugee and Aboriginal and Torres Strait Islander families to access mental health and wellbeing information, given that almost all children and families come into contact with them.
Schools must continue to create and maintain a supportive environment for promoting the wellbeing of all students (action 3.1.f) led by the wellbeing coordinator. This can be achieved via specific programs such as Think Equal, which have been designed to promote social and emotional learning and to reduce gender inequality, racism and other divisive behaviours via increasing compassion, empathy and critical thinking. In some cases, coordinators will be able to identify tailored activities to suit the profile of their school community. For example, a school with a high proportion of Aboriginal and Torres Strait Islander students might choose to develop a Reconciliation Action Plan in order to build cultural safety of learning environments and to ensure the social and emotional wellbeing of the students and their families.
There is also further opportunity to promote early social and emotional development in early childhood learning services. A 2018 review of the quality of evidence for preschool programs to support social and emotional skills found four programs with high-quality evidence of impacts. Positive outcomes included impact on social behaviours, conduct problems, emotional distress and parent-child interactions. Accredited social and emotional wellbeing programs which are appropriate for pre-school age children need to be delivered through early childhood education settings, including programs that assist children to develop skills to relate with other peers and regulate their emotions (action 3.1.g). Programs for school aged children should also be available after school and during school holidays to provide respite to parents and to help children with emotional wellbeing, loneliness, and self-worth (action 3.1.h).
Things we can build on
The Alice Springs (Mparntwe) Education Declaration (signed in Dec 2019), sets out the national vision for education and the commitment of Australian Governments to improving educational outcomes. The Declaration places students at the centre of their education by emphasising the importance of meeting the individual needs of all learners, and outlines education’s role in supporting the wellbeing, mental health and resilience of young people.
The National Quality Standard (NQS) sets a high national benchmark for early childhood education and care and outside school hours care services in Australia. Under the National Law and Regulations, all early childhood education and care services are required to base their educational program on an approved learning framework. Belonging, Being and Becoming: The Early Years Learning Framework for Australia is the approved learning framework under the NQS for young children from birth to five years of age. My Time, Our Place: Framework for School Age Care in Australia is the approved learning framework under the NQS for school age children. These frameworks encompass social and emotional wellbeing and development outcomes.
Be You is a universal mental health and wellbeing program for children that can be delivered in schools and early childhood learning services. It was established through the integration of a number of Australian Government funded programs, combining knowledge and expertise gained from these over the years. Be You provides a common framework with evidenced-based information, professional advice and support for educators. Be You is also delivering whole-of-team professional learning to more than 3,000 early childhood learning services, aiming to reach all 15,000 services eventually. Be You is being implemented in 70% of schools nationally.
The Student Wellbeing Hub is an online platform that aims is to support Australian schools to promote student wellbeing, safety, and positive relationships. The Hub is underpinned by the Australian Student Wellbeing Framework (2018). The Hub provides high-quality, age-appropriate information and resources targeted specifically to educators, parents and students. The educator area contains free, self-paced and certificated professional learning courses on a range of key topics for schools. The parent area contains advice, information and guides to support them navigate their children’s journey through school. Students can access games, quizzes and information about issues most important to them.
A Mental Health in Primary Schools Pilot (MHiPS) is a project commenced in a number of Victorian schools in 2020. Based on a needs analysis, a literature review, and discussions with key stakeholders, a Mental Health and Wellbeing Coordinator (MHWC) role was designed. The MHWC, who is from an education background, is tasked with building the capability of the whole school with regard to mental health and wellbeing, providing support to staff to better identify and support students with mental health needs, establishing clear pathways for referral for students requiring assessment and intervention, monitoring and evaluating student progress, and promoting connections between the education and health sectors. To provide the MHWCs with training appropriate for the role, a 3-day intensive, online synchronous training program was delivered. MHWCs are then supported throughout the year with community of practice sessions and ongoing supervision, which aim to build the practical skills of the trainees along with giving them space to reflect on the real world implementation of their learnings.
Targeted programs for children who have experienced significant change or loss in their lives are based on the principles of normalising emotions in response to difficult experiences. They help children to understand their feelings, learn skills that help them adapt, and develop reciprocal friendships which reduce isolation - ‘I’m not the only one who this has happened to’. Evaluations of this model of psychoeducation coupled with peer support have found that the majority of children respond positively to the learning outcomes, including increased confidence in seeking support, general feelings of coping better and being able to talk about feelings more freely.
The National Principles for Child Safe Organisations were agreed by all Australian governments in February 2019. They are 10 high-level principles that set out a nationally consistent approach to promoting a culture of child safety and wellbeing within organisations, including educational settings such as schools and early childcare institutions. The National Principles highlight the importance of involving children in decisions that affect them, creating safe environments that support both physical and emotional safety, and creating child focused complaints processes so children feel comfortable raising concerns when they feel unhappy, uncomfortable or unsafe. The National Office for Child Safety leads development of resources to assist organisations to implement the National Principles.
Actions 3.1
a. Conduct thorough reviews of school and early childhood policies and processes, looking for opportunities to reduce possible stigma and discrimination.
b. Identify senior staff within early childhood learning services to be responsible for (1) planning and coordinating wellbeing activities for the students, and (2) maintaining knowledge of and relationships with locally available and online supports.
c. Employ wellbeing coordinators in each primary school to be responsible for (1) planning and coordinating wellbeing activities for the students, and (2) maintaining knowledge of and relationships with locally available and online supports. These positions should be funded on an ongoing basis.
d. Identify opportunities to incorporate conversations about mental health and wellbeing into the school or early childhood daily routines, with the expectation that all staff and students have the opportunity to contribute to these discussions.
e. Promote evidence-based, locally available or online supports and services to children and families through schools and early childhood learning services.
f. Outline and regularly report on how schools and early childhood learning services are improving on current levels of cultural accessibility for children who identify as Aboriginal or Torres Strait Islander or from culturally and linguistically diverse backgrounds.
g. Implement evidence-based wellbeing programs within schools and early childhood learning services, with support from existing initiatives such as Be You.
h. Increase accessible activities after school and during school holidays to provide respite for parents and children.
Objective 3.2 Targeted responses
All early childhood learning services and schools should have a wellbeing plan in place for their students, with policies and processes developed or adapted to address the gaps in support identified as part of wellbeing planning (action 3.2.a). This should be based on an audit of policies and processes to examine whether they are effective in delivering wellbeing outcomes for students. For early childhood learning services, this could be through adding mental health to Quality Improvement Plans to avoid duplication in planning processes. Flexible funding must be available to schools and early childhood learning services for the purpose of improving policies and processes and ensuring high fidelity program implementation. This funding should be allocated based on need, with funds available specifically for quality improvement activities (action 3.2.b), and for implementation of evidence-based psychosocial and therapeutic supports (action 3.2.c).
At primary school stage, a common issue raised by both parents and educators relates to bullying, which has been the subject of much research. There is evidence that children who are bullied by peers have an increased risk of problems in young adulthood including anxiety, depression, self-harm and suicidality.180 Racism is also occurring in education settings, with 40% of Indigenous children aged 4–14 years reporting that they been bullied at school and 9% had been treated unfairly at school because they were Aboriginal and/or Torres Strait Islander. Children can be bullied and experience racism both inside and outside of the school environment, including online.
Schools should deliver programs to assist with the prevention of bullying and racism, and to support healthy peer relationships (action 3.2.c). However, as is the case with wellbeing programs generally, there is currently a wide variety of programs available for schools, but not all are evidence-based or implemented as intended. Full implementation of programs is often difficult due to the competing demands on a teacher’s time and curriculum space, but an evidence-based program needs to be implemented with fidelity to achieve the intended benefits. One function of the wellbeing staff (action 3.1.c) would be to ensure selection of programs that have been accredited as evidence-based, and to oversee their implementation.
A key aspect of how educators should respond when concerned about a student’s wellbeing is to discuss their impressions with the parents. Conversations between educators and families are important as both have an opportunity to observe children in a different context from the other, which provides useful insights into why a child might be struggling and how they can be best supported. Schools and early childhood education centres need specific strategies and tools to discuss mental health concerns with parents. These may be adapted from materials that address more generic communication, such as Raising Children Network’s ‘effective communication’ series which provides guidance for professionals on communicating with parents, and guidance for teachers on encouraging parental involvement in school (action 3.2.d).
School engagement and mental health are also linked, with mental illness often a major reason for disengagement from education and a significant barrier to returning to school. School disengagement can occur at different levels, and while it is less common in primary than in high schools, up to 18% of primary school students attend less than 90% of the time. Disengagement from education is not always as obvious as a child being physically absent from the classroom. They could be disengaged in the content of the lesson, or with the particular class or teacher, or with school as a whole. At all levels, disengagement presents a risk for the child’s educational attainment. This in turn has downstream impacts on later likelihood of employment, low income, social exclusion, risky health behaviours (such as smoking and alcohol abuse) and engaging in crime, all of which contribute to greater likelihood of development of mental illness.
Young people reported that when their school engagement was disrupted by challenges they were experiencing in their home environment (for example, they were frequently late or missed school), the school would often respond with punishment instead of trying to understand what the issues were and how they could be accommodated. Schools and educators need support to develop procedures for proactive outreach to be automatically triggered when a student’s attendance declines below a pre-determined level. In addition to reviewing school disciplinary policies and practices (action 3.1.a), primary school educators would benefit from additional opportunities to consider how they respond to student disengagement and behavioural issues.
This is in line with the Productivity Commission’s recommendationsm, and the 2020 Review of the Disability Standards for Education (2005) which highlighted the need to strengthen the capability of educators and providers to support students with a disability, and to embed accountability for the Standards throughout the education system. In an effort to move away from punitive disciplinary responses, these instances should trigger consideration of the child’s mental health and a care plan should be developed in collaboration with both the child and their family. Similarly, early childhood educators must be supported to adopt a trauma-informed approach when children and families are disengaging from their service (action 3.2.e).
In the preschool years, early childhood education can be an avenue to address social disadvantage, including as a way of helping vulnerable children reach their full potential, and to reduce intergenerational cycles of poverty and incarceration but not all children and families access it. While the Commonwealth Department of Education has a Child Care Safety Net to provide additional assistance to services looking after the most vulnerable children, only a third of the anticipated 70,000 low-income families expected to access these entitlements have actually done so. The GAP Taskforce on Early Childhood Education identified that the factors affecting families’ lack of participation are more complex than access to funding or facilities. Their findings indicated that integrating health, welfare, school and early learning on the same site improves outcomes, along with engaging local communities to encourage use of these services.
Things we can build on
Several State and Territory Education Departments have Student Wellbeing Plans. Some schools are choosing to implement programs that focus on key issues such as bullying. There are strong examples of school-based child welfare programs that have been designed to be delivered in mainstream schools to cater for students needing complex educational and therapeutic support. Programs are delivered to educators via structured professional development, consultation and mentoring, and are based on the rationale that children’s biological and developmental responses to trauma need to be addressed before they can engage with learning content.
The Commonwealth Department of Education’s Inclusion Support Program provides additional support for children that need it, and the guidelines have been expanded to include children who are not coping, are struggling, or unwell. The Inclusion Support Program’s objectives are to:
support eligible mainstream Early Childhood Education and Care (ECEC) services to improve their capacity and capability to provide quality inclusive practices for all children
address access and participation barriers and to support the inclusion of children with additional needs
provide parents or carers of children with additional needs with access to appropriate and inclusive ECEC services so parents or carers can increase their activity including work, study and training.
Research indicates that students from disadvantaged backgrounds profit most from a combination of whole-of-school and targeted programs. The evidence also suggests that specific student belonging and engagement programs in schools had the greatest impact on academic achievement. A pilot program, Thriving Together is currently underway in NSW. Based on a social prescribing framework, the program is designed to promote the benefit of early learning to families living in poverty and to break down the barriers to early learning and childhood care. It has been designed to create a wraparound inter-agency response to support the ‘front line’ parent(s), and to support GPs with an easier referral pathway to access external services and reduce demand on primary care.
Actions 3.2
a. Require all early childhood learning services and primary schools to develop a comprehensive wellbeing plan, which should outline what the service or school will do to address issues identified as a priority for their students (including those identified as part of actions 3.1.a and 4.1.c). Progress against these plans should be reported on regularly.
b. Make funds available for schools to implement quality improvement activities related to student mental health and wellbeing.
c. Make funds available for schools to deliver evidence-based programs targeting the needs identified as part of action 3.2.a, with a particular focus on bullying and racism.
d. Adapt existing resources and training programs to provide educators with the skills to discuss mental health concerns about a child/student with their parents or carers, including provision of interpreting services where necessary.
e. Establish and implement trauma-informed procedures for responding to students disengaging from education.
Objective 3.3 Well-equipped educators
Educators are uniquely positioned to identify signs when children are struggling and to facilitate their connection with supports. However, they are not always provided with the knowledge or support to ensure they are capable and confident to do this effectively. Amongst educators, there is variability in awareness of the signs that children are struggling or not meeting social and emotional developmental milestones. Educators also experience difficulties identifying the threshold at which they should seek additional support for a child and are not always confident raising concerns if they were not first raised by a parent.
Despite this, there is interest amongst educators in improving understanding of how children’s mental health and wellbeing can be supported in the classroom. There is a need to develop professional teacher training (action 3.3.a) on key topics such as:
Identification of early warning signs that a child is struggling with their mental health and where to refer families when necessary
How to have effective conversations with children and parents about a child’s wellbeing
Appreciation of the broader Social and Emotional Wellbeing concept for Aboriginal and Torres Strait Islander communities
Trauma-informed approaches to education.
There is also a need to have clear guidelines and processes in place, for educators to follow when they suspect a child or family are struggling. This is likely to be involving the student wellbeing coordinator as the first step (action 3.3.b). Wellbeing coordinators also require sufficient education and training to perform their role (action 3.3.c).
Educators play an important role as informed members of management teams, including to implement support plans in the school environment. In the first instance, educators should be aware of the range of options for children and families to seek mental health and wellbeing supports (action 3.3.b). This includes supports and services provided through the school and the local community, as well as state or nation-wide services. This may be achieved through professional development training and staff meeting/induction processes.
In order for the child to receive the support they need, treatment plans depend on educators being able to develop effective working relationships with external health providers as well as parents. Wellbeing staff should have responsibility for establishing and maintaining strong relationships with local service providers including paediatricians, psychologists, allied health professionals including speech pathologists and occupational therapists, community health centres, and mental health services. This could be facilitated through a designated contact within the service who is known to (and works with) the school staff with wellbeing responsibilities (action 3.1.c, action 3.3.b).
In order for educators to be able to support students and their families, educators’ mental health and wellbeing needs to be supported. Without this support, educators are at greater risk of feeling burnt out and experiencing their own mental health struggles. Most State and Territory Education Departments have targeted wellbeing plans for teachers and/or principals, recognising that positive wellbeing contributes to increased job satisfaction, enhanced leadership, and improved delivery of quality teaching and learning for students. While there are programs such as Employee Assistance Programs, these are not available to all educators. Wellbeing staff should promote relevant staff training on mental health and wellbeing, including policies, procedures and information about available services for staff and students both internally and externally, such as support via an educator’s regular GP (action 3.3.d).
While educators have diverse roles and cannot be expected to have the same level of expertise in mental health as mental health professionals, a minimum standard of professional development in relation to child mental health should be applied (action 3.3.e). For example, educators could be required to complete accredited professional development relating to mental health or wellbeing once every two years. Professional development should be accredited according to national guidelines and paid protected time should be available for completion of professional development activities.
Things we can build on
The Australian Professional Standards for Teachers set out what teachers should be aiming to achieve at every stage of their career. These include creating and maintaining supportive and safe learning environments, engaging in professional learning, and engaging professionally with colleagues, parents/carers and the community.
Programs are available for primary schools to help make it easier for educators to identify children who are struggling, in order to offer them school-based interventions and/or external referrals. One model is based on training educators in the following: noticing changes in mood or behaviour (that may indicate difficulties in managing emotional distress), building trusting and supportive relationships with parents and carers, inquiring sensitively about the child’s circumstances, and planning the first steps and referrals within or outside the school setting.
One consequence of the move to home-based learning as a result of the recent pandemic, has been increased opportunities for communication with parents. This had strengthened the relationship between teacher and families and has given some parents and carers a new appreciation for the strengths and difficulties their children have in different domains. A similar advantage has been seen with the introduction of telehealth measures, which have increased opportunities for health professionals to connect with educators to support children in their care.
Actions 3.3
a. Develop professional learning courses/modules specifically designed for educators that focus on key mental health and wellbeing topics.
b. Create clear processes to guide educators when concerned about the mental health of a student/child, including up-to-date information regarding the range of locally available or online support options for children and families (note role of wellbeing coordinators, see action 3.1.c).
c. Provide designated wellbeing coordinator staff (see action 3.1.c) with appropriate training to undertake their role.
d. Ensure formal, independent mental health and wellbeing supports are made available to all educators for their own mental health and wellbeing, building on existing teacher and principal wellbeing plans and frameworks.
e. Establish professional learning requirements for educators in relation to mental health, with paid protected time for participation.
The below table outlines some proposed indicators of change. If the objectives of this focus area are realised, we would expect to see improvements in the below.
Focus Area 3: Education Settings – indicators of change
3.1. Use of policies, processes and programs supporting child mental health and wellbeing
3.2. Proportion of education institutions with wellbeing coordinators
3.3. Uptake of training and professional development in child mental health and wellbeing
Last updated:
Acknowledgement of Country
The Commission acknowledges Aboriginal and Torres Strait Islander peoples as the Traditional Custodians of the lands and waters on which we live, work and learn.
Diversity
The Commission is committed to embracing diversity and eliminating all forms of discrimination in the provision of health services. The Commission welcomes all people irrespective of ethnicity, lifestyle choice, faith, sexual orientation and gender identity.
Lived Experience
We acknowledge the individual and collective contributions of those with a lived and living experience of mental ill-health and suicide, and those who love, have loved and care for them. Each person’s journey is unique and a valued contribution to Australia’s commitment to mental health suicide prevention systems reform.